Ploutarchos Tzoulis, Gregory Kaltsas, Stephanie E Baldeweg, Pierre-Marc Bouloux, Ashley B Grossman
{"title":"Tolvaptan for the treatment of the syndrome of inappropriate antidiuresis (SIAD).","authors":"Ploutarchos Tzoulis, Gregory Kaltsas, Stephanie E Baldeweg, Pierre-Marc Bouloux, Ashley B Grossman","doi":"10.1177/20420188231173327","DOIUrl":null,"url":null,"abstract":"<p><p>The syndrome of inappropriate antidiuresis (SIAD), the commonest cause of hyponatraemia, is associated with significant morbidity and mortality. Tolvaptan, an oral vasopressin V2-receptor antagonist, leads through aquaresis to an increase in serum sodium concentration and is the only medication licenced in Europe for the treatment of euvolaemic hyponatraemia. Randomised controlled trials have shown that tolvaptan is highly efficacious in correcting SIAD-related hyponatraemia. Real-world data have confirmed the marked efficacy of tolvaptan, but they have also reported a high risk of overly rapid sodium increase in patients with a very low baseline serum sodium. The lower the baseline serum sodium, the higher the tolvaptan-induced correction rate occurs. Therefore, a lower starting tolvaptan dose of 7.5 mg has been evaluated in small cohort studies, demonstrating its efficacy, but it still remains unclear as to whether it can reduce the risk of overcorrection. Most international guidelines, except for the European ones, recommend tolvaptan as second-line treatment for SIAD after fluid restriction. However, the risk of unduly rapid sodium correction in combination with its high cost have limited its routine use. Prospective controlled studies are warranted to evaluate whether tolvaptan-related sodium increase can improve patient-related clinical outcomes, such as mortality and length of hospital stay in the acute setting or neurocognitive symptoms and quality of life in the chronic setting. In addition, the potential role of a low tolvaptan starting dose needs to be further explored. Until then, tolvaptan should mainly be used as second-line treatment for SIAD, especially when there is a clinical need for prompt restoration of normonatraemia. Tolvaptan should be used with specialist input according to a structured clinical pathway, including rigorous monitoring of electrolyte and fluid balance and, if needed, implementation of appropriate measures to prevent, or when necessary reverse, overly rapid hyponatraemia correction.</p>","PeriodicalId":22998,"journal":{"name":"Therapeutic Advances in Endocrinology and Metabolism","volume":"14 ","pages":"20420188231173327"},"PeriodicalIF":4.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c5/c1/10.1177_20420188231173327.PMC10192810.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Endocrinology and Metabolism","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420188231173327","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
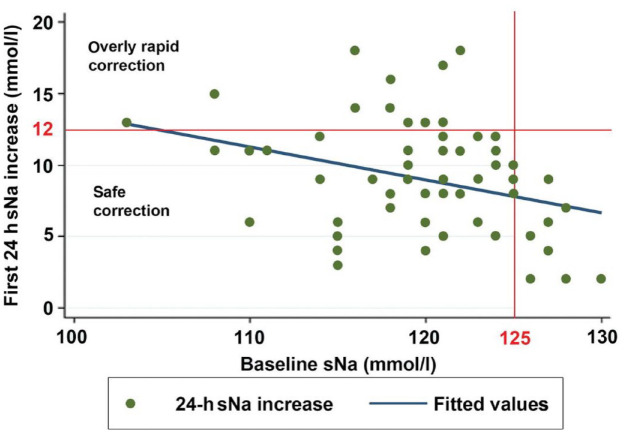
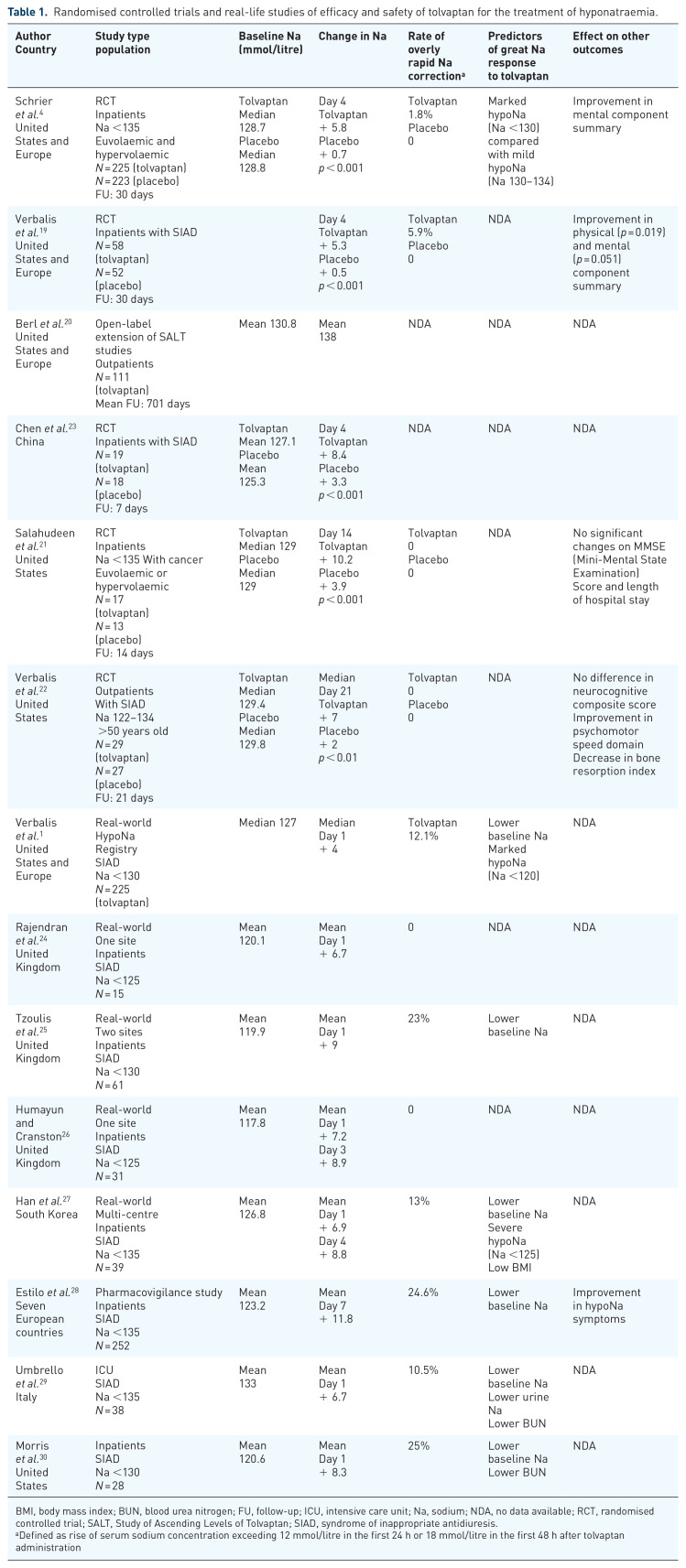
The syndrome of inappropriate antidiuresis (SIAD), the commonest cause of hyponatraemia, is associated with significant morbidity and mortality. Tolvaptan, an oral vasopressin V2-receptor antagonist, leads through aquaresis to an increase in serum sodium concentration and is the only medication licenced in Europe for the treatment of euvolaemic hyponatraemia. Randomised controlled trials have shown that tolvaptan is highly efficacious in correcting SIAD-related hyponatraemia. Real-world data have confirmed the marked efficacy of tolvaptan, but they have also reported a high risk of overly rapid sodium increase in patients with a very low baseline serum sodium. The lower the baseline serum sodium, the higher the tolvaptan-induced correction rate occurs. Therefore, a lower starting tolvaptan dose of 7.5 mg has been evaluated in small cohort studies, demonstrating its efficacy, but it still remains unclear as to whether it can reduce the risk of overcorrection. Most international guidelines, except for the European ones, recommend tolvaptan as second-line treatment for SIAD after fluid restriction. However, the risk of unduly rapid sodium correction in combination with its high cost have limited its routine use. Prospective controlled studies are warranted to evaluate whether tolvaptan-related sodium increase can improve patient-related clinical outcomes, such as mortality and length of hospital stay in the acute setting or neurocognitive symptoms and quality of life in the chronic setting. In addition, the potential role of a low tolvaptan starting dose needs to be further explored. Until then, tolvaptan should mainly be used as second-line treatment for SIAD, especially when there is a clinical need for prompt restoration of normonatraemia. Tolvaptan should be used with specialist input according to a structured clinical pathway, including rigorous monitoring of electrolyte and fluid balance and, if needed, implementation of appropriate measures to prevent, or when necessary reverse, overly rapid hyponatraemia correction.
期刊介绍:
Therapeutic Advances in Endocrinology and Metabolism delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of endocrinology and metabolism.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
