{"title":"Collateral circulation status-guided mechanical thrombectomy in pediatric stroke with an extended ghost infarct core: illustrative case.","authors":"Tian-Min Lai, Kun-Xin Lin, Ying Fu, Ling Fang, Wen-Long Zhao","doi":"10.3171/CASE22404","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mechanical thrombectomy (MT) has been proved to be a highly effective therapy to treat acute ischemic stroke due to large vessel occlusion. Often, the ischemic core extent on baseline imaging is an important determinant for endovascular treatment eligibility. However, computed tomography (CT) perfusion (CTP) or diffusion-weighted imaging may overestimate the infarct core on admission and, consequently, smaller infarct lesions called \"ghost infarct cores.\"</p><p><strong>Observations: </strong>A 4-year-old, previously healthy boy presented with acute-onset, right-sided weakness and aphasia. Fourteen hours after the onset of symptoms, the patient presented with a National Institutes of Health Stroke Scale (NIHSS) score of 22, and magnetic resonance angiography demonstrated a left middle cerebral artery occlusion. MT was not considered because of a large infarct core (infarct core volume: 52 mL; mismatch ratio 1.6 on CTP). However, multiphase CT angiography indicated good collateral circulation, which encouraged MT. Complete recanalization was achieved via MT at 16 hours after the onset of symptoms. The child's hemiparesis improved. Follow-up magnetic resonance imaging was nearly normal and showed that the baseline infarct lesion was reversible, in agreement with neurological improvement (NIHSS score 1).</p><p><strong>Lessons: </strong>The selection of pediatric stroke with a delayed time window guided by good collateral circulation at baseline seems safe and efficacious, which suggests a promising value of vascular window.</p>","PeriodicalId":16554,"journal":{"name":"Journal of Neurosurgery: Case Lessons","volume":"5 20","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/36/d3/CASE22404.PMC10550523.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurosurgery: Case Lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE22404","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Mechanical thrombectomy (MT) has been proved to be a highly effective therapy to treat acute ischemic stroke due to large vessel occlusion. Often, the ischemic core extent on baseline imaging is an important determinant for endovascular treatment eligibility. However, computed tomography (CT) perfusion (CTP) or diffusion-weighted imaging may overestimate the infarct core on admission and, consequently, smaller infarct lesions called "ghost infarct cores."
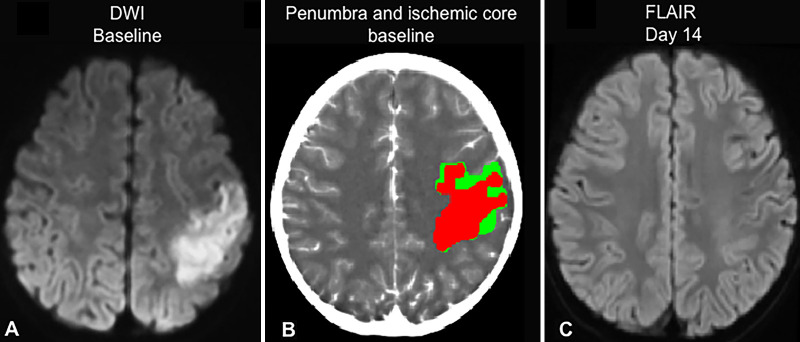
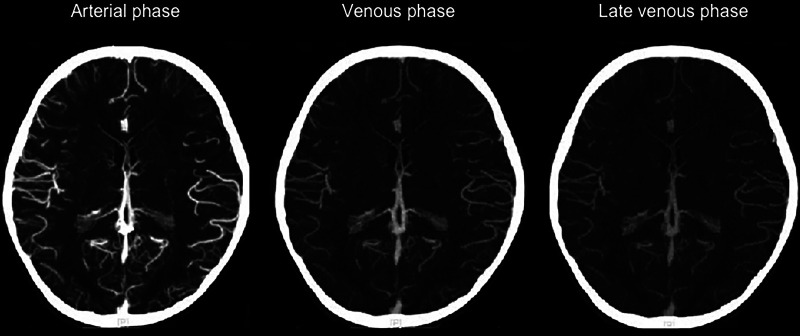
Observations: A 4-year-old, previously healthy boy presented with acute-onset, right-sided weakness and aphasia. Fourteen hours after the onset of symptoms, the patient presented with a National Institutes of Health Stroke Scale (NIHSS) score of 22, and magnetic resonance angiography demonstrated a left middle cerebral artery occlusion. MT was not considered because of a large infarct core (infarct core volume: 52 mL; mismatch ratio 1.6 on CTP). However, multiphase CT angiography indicated good collateral circulation, which encouraged MT. Complete recanalization was achieved via MT at 16 hours after the onset of symptoms. The child's hemiparesis improved. Follow-up magnetic resonance imaging was nearly normal and showed that the baseline infarct lesion was reversible, in agreement with neurological improvement (NIHSS score 1).
Lessons: The selection of pediatric stroke with a delayed time window guided by good collateral circulation at baseline seems safe and efficacious, which suggests a promising value of vascular window.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
