{"title":"The Validity of Heart Rate Variability Obtained from Electrocardiography and Blood Pressure in Rats Subjected to Isoproterenol-Induced Heart Ischemia.","authors":"Maryam Farokhipour, Farzaneh Ketabchi","doi":"10.18502/jthc.v18i1.12579","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Heart rate variability (HRV) is calculated by electrocardiography (ECG-HRV) or blood pressure (BP-HRV). The purpose of this study was to determine the validity of the above methods in rats with normal and ischemic hearts during the baroreflex maneuver.</p><p><strong>Methods: </strong>The study was conducted at Shiraz University of Medical Sciences, Shiraz, Iran, in 2021. Sprague-Dawley rats were divided into a sham group and an isoproterenol-mediated cardiac ischemia (ISO) group. Saline and isoproterenol (150 mg/kg) injected subcutaneously for 2 consecutive days in the sham and ISO groups, respectively. Then, the animals were anesthetized with an intraperitoneal injection of sodium thiopental (60 mg/kg), and the femoral artery and vein were cannulated. Baroreflex was activated using an intravenous injection of phenylephrine (10 μg/100 μL saline). ECG, BP, and heart rate (HR) were recorded, and the time domain of HRV and baroreflex gain were calculated.</p><p><strong>Results: </strong>Baroreflex gain in the ISO group (male, weight=275.8±2.8 g, n=8) was lower than that in the sham group (male, weight=258±2.3 g, n=8) (P<0.05). ECG-HRV indicated an increase in the standard deviation of the RR interval (SDRR), the index of overall HRV, and the parasympathetic index of the root mean square of successive differences (RMSSD) in both groups. However, the rise in SDRR and RMSSD in the ISO group was less than that in the sham group (P<0.05). SDRR and RMSSD obtained from BP did not show a difference between the sham and ISO groups, nor did they correspond with the results seen in baroreflex gain.</p><p><strong>Conclusion: </strong>BP-HRV was not as valuable as ECG-HRV in assessing cardiac ischemia.</p>","PeriodicalId":39149,"journal":{"name":"Journal of Tehran University Heart Center","volume":"18 1","pages":"33-38"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/11/6d/JTHC-18-33.PMC10225032.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Tehran University Heart Center","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jthc.v18i1.12579","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Heart rate variability (HRV) is calculated by electrocardiography (ECG-HRV) or blood pressure (BP-HRV). The purpose of this study was to determine the validity of the above methods in rats with normal and ischemic hearts during the baroreflex maneuver.
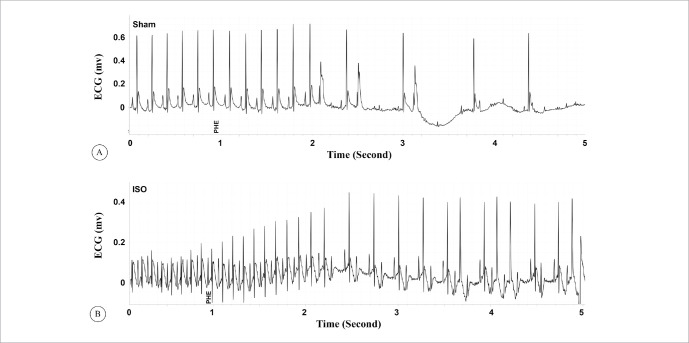
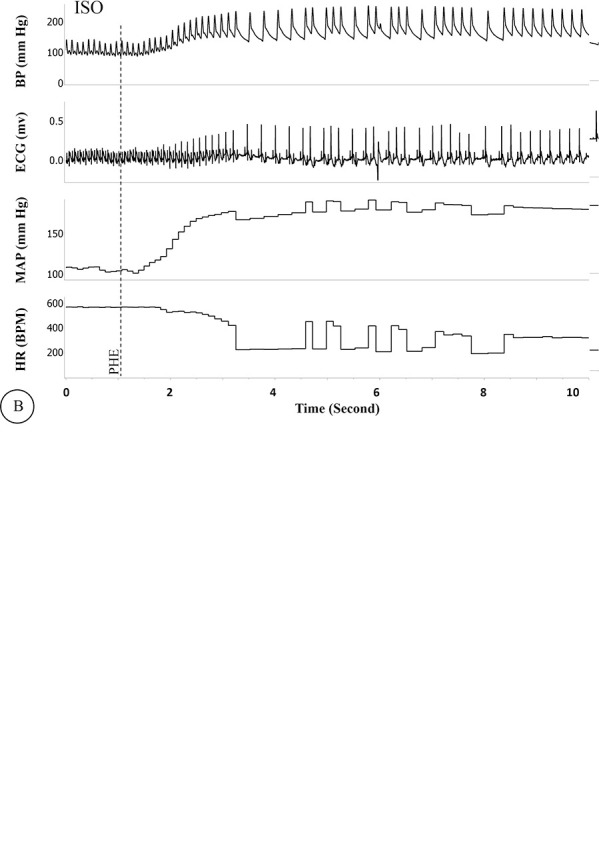
Methods: The study was conducted at Shiraz University of Medical Sciences, Shiraz, Iran, in 2021. Sprague-Dawley rats were divided into a sham group and an isoproterenol-mediated cardiac ischemia (ISO) group. Saline and isoproterenol (150 mg/kg) injected subcutaneously for 2 consecutive days in the sham and ISO groups, respectively. Then, the animals were anesthetized with an intraperitoneal injection of sodium thiopental (60 mg/kg), and the femoral artery and vein were cannulated. Baroreflex was activated using an intravenous injection of phenylephrine (10 μg/100 μL saline). ECG, BP, and heart rate (HR) were recorded, and the time domain of HRV and baroreflex gain were calculated.
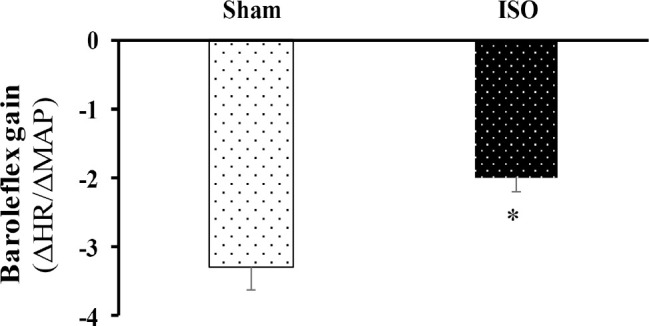
Results: Baroreflex gain in the ISO group (male, weight=275.8±2.8 g, n=8) was lower than that in the sham group (male, weight=258±2.3 g, n=8) (P<0.05). ECG-HRV indicated an increase in the standard deviation of the RR interval (SDRR), the index of overall HRV, and the parasympathetic index of the root mean square of successive differences (RMSSD) in both groups. However, the rise in SDRR and RMSSD in the ISO group was less than that in the sham group (P<0.05). SDRR and RMSSD obtained from BP did not show a difference between the sham and ISO groups, nor did they correspond with the results seen in baroreflex gain.
Conclusion: BP-HRV was not as valuable as ECG-HRV in assessing cardiac ischemia.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
