Conventional outcome reporting per IVF cycle/embryo transfer may systematically underestimate chances of success for women undergoing ART: relevant biases in registries, epidemiological studies, and guidelines.
{"title":"Conventional outcome reporting per IVF cycle/embryo transfer may systematically underestimate chances of success for women undergoing ART: relevant biases in registries, epidemiological studies, and guidelines.","authors":"Georg Griesinger, Per Larsson","doi":"10.1093/hropen/hoad018","DOIUrl":null,"url":null,"abstract":"<p><p>Pre-conception counselling and management of expectations about chance of success of IVF/ICSI treatments is an integral part of fertility care. Registry data are usually used to inform patients about expected success rates of IVF/ICSI treatment, as these data should best represent real-world populations and clinical practice. In registries, the success rate of IVF/ICSI treatments is conventionally reported per treatment cycle or per embryo transfer and estimated from data for which several treatment attempts per subject have been pooled (e.g. repetitive IVF/ICSI attempts or repetitive attempts of cryotransfer). This, however, may underestimate the true mean chance of success per treatment attempt, because treatment attempts of women with a poor prognosis will usually be over-represented in a pool of treatment cycle data compared to treatment events of women with a good prognosis. Of note, this phenomenon is also a source of potential bias when comparing outcomes between fresh transfers and cryotransfers, since women can undergo a maximum of only one fresh transfer after each IVF/ICSI treatment, but potentially several cryotransfers. Herein, we use a trial dataset from 619 women, who underwent one cycle of ovarian stimulation and ICSI, a Day 5 fresh transfer and/or subsequent cryotransfers (follow-up of all cryotransfers up to 1 year after the start of stimulation), to exemplify the underestimation of the live birth rate, when not accounting for repeated transfers in the same woman. Using mixed-effect logistic regression modelling, we show that the mean live birth rate per transfer per woman in cryocycles is underestimated by the factor 0.69 (e.g. live birth rate per cryotransfer of 36% after adjustment versus 25% unadjusted). We conclude that the average chance of success of treatment cycles of women of a given age, treated in a given centre, etc., when conventionally calculated per cycle or per embryo transfer from a pool of treatment events, do not apply to an individual woman. We suggest that patients are, especially at the outset of treatment, systematically confronted with mean estimates of success per attempt that are too low. Live birth rates per transfer from datasets encompassing multiple transfers from single individuals could be more accurately reported using statistical models accounting for the correlation between cycle outcomes within women.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2023 2","pages":"hoad018"},"PeriodicalIF":11.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9d/37/hoad018.PMC10214861.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoad018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
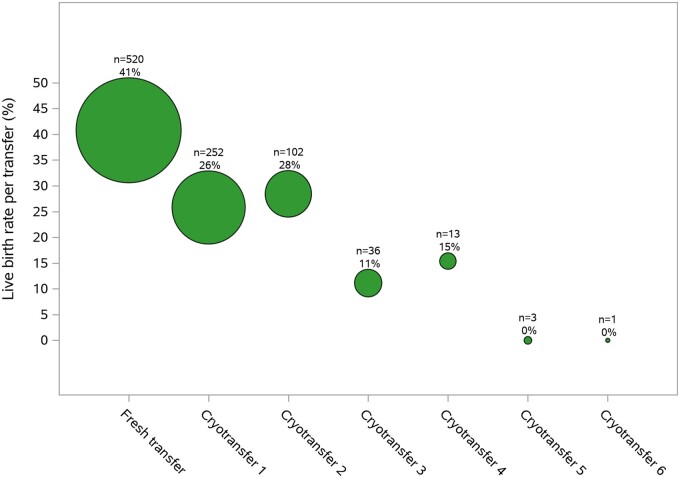
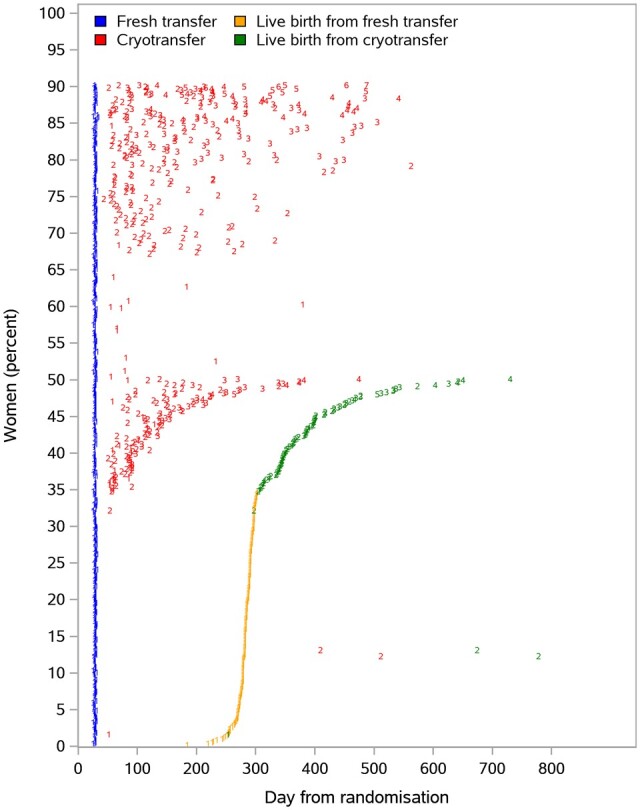
Pre-conception counselling and management of expectations about chance of success of IVF/ICSI treatments is an integral part of fertility care. Registry data are usually used to inform patients about expected success rates of IVF/ICSI treatment, as these data should best represent real-world populations and clinical practice. In registries, the success rate of IVF/ICSI treatments is conventionally reported per treatment cycle or per embryo transfer and estimated from data for which several treatment attempts per subject have been pooled (e.g. repetitive IVF/ICSI attempts or repetitive attempts of cryotransfer). This, however, may underestimate the true mean chance of success per treatment attempt, because treatment attempts of women with a poor prognosis will usually be over-represented in a pool of treatment cycle data compared to treatment events of women with a good prognosis. Of note, this phenomenon is also a source of potential bias when comparing outcomes between fresh transfers and cryotransfers, since women can undergo a maximum of only one fresh transfer after each IVF/ICSI treatment, but potentially several cryotransfers. Herein, we use a trial dataset from 619 women, who underwent one cycle of ovarian stimulation and ICSI, a Day 5 fresh transfer and/or subsequent cryotransfers (follow-up of all cryotransfers up to 1 year after the start of stimulation), to exemplify the underestimation of the live birth rate, when not accounting for repeated transfers in the same woman. Using mixed-effect logistic regression modelling, we show that the mean live birth rate per transfer per woman in cryocycles is underestimated by the factor 0.69 (e.g. live birth rate per cryotransfer of 36% after adjustment versus 25% unadjusted). We conclude that the average chance of success of treatment cycles of women of a given age, treated in a given centre, etc., when conventionally calculated per cycle or per embryo transfer from a pool of treatment events, do not apply to an individual woman. We suggest that patients are, especially at the outset of treatment, systematically confronted with mean estimates of success per attempt that are too low. Live birth rates per transfer from datasets encompassing multiple transfers from single individuals could be more accurately reported using statistical models accounting for the correlation between cycle outcomes within women.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
