John A Elefteriades, Bulat A Ziganshin, Mohammad A Zafar
{"title":"Nonsize Criteria for Surgical Intervention on the Ascending Thoracic Aorta.","authors":"John A Elefteriades, Bulat A Ziganshin, Mohammad A Zafar","doi":"10.1055/s-0043-1766114","DOIUrl":null,"url":null,"abstract":"<p><p>For decades, aortic surgery has relied on size criteria for intervention on the ascending aorta. While diameter has served well, diameter alone falls short of an ideal criterion. Herein, we examine the potential application of other, nondiameter criteria in aortic decision-making. These findings are summarized in this review. We have conducted multiple investigations of specific alternate nonsize criteria by leveraging our extensive database, which includes complete, verified anatomic, clinical, and mortality data on 2,501 patients with thoracic aortic aneurysm (TAA) and dissections (198 Type A, 201 Type B, and 2102 TAAs). We examined 14 potential intervention criteria. Each substudy had its own specific methodology, reported individually in the literature. The overall findings of these studies are presented here, with a special emphasis on how the findings can be incorporated into enhanced aortic decision-making-above and beyond sheer diameter. The following nondiameter criteria have been found useful in decision-making regarding surgical intervention. (1) Pain: In the absence of other specific cause, substernal chest pain mandates surgery. Well-developed afferent neural pathways carry warning signals to the brain. (2) Aortic length/tortuosity: Length is emerging as a mildly better predictor of impending events than diameter. (3) Genes: Specific genetic aberrations provide a powerful predictor of aortic behavior; malignant genetic variants obligate earlier surgery. (4) Family history: Aortic events closely follow those in relatives with a threefold increase in likelihood of aortic dissection for other family members once an index family dissection has occurred. (5) Bicuspid aortic valve: Previously thought to increase aortic risk (as a \"Marfan light\" situation), current data show that bicuspid valve is not a predictor of higher risk. (6) Diabetes actually protects against aortic events, via mural thickening and fibrosis. (7) Biomarkers: A specialized \"RNA signature test\" identifies aneurysm-bearing patients in the general population and promises to predict impending dissection. (8) Aortic stress: Blood pressure (BP) elevation from anxiety/exertion precipitates dissection, especially with high-intensity weightlifting. (9) Root dilatation imposes higher dissection risk than supracoronary ascending aneurysm. (10) Inflammation on positron emission tomography (PET) imaging implies high rupture risk and merits surgical intervention. (11) A <i>KIF6</i> p.Trp719Arg variant elevates aortic dissection risk nearly two-fold. (12) Female sex confers some increased risk, which can be largely accommodated by using body-size-based nomograms (especially height nomograms). (13) Fluoroquinolones predispose to catastrophic dissection events and should be avoided rigorously in aneurysm patients. (14) Advancing age makes the aorta more vulnerable, increasing likelihood of dissection. In conclusion, nondiameter criteria can beneficially be brought to bear on the decision to observe or operate on specific TAA.</p>","PeriodicalId":72248,"journal":{"name":"","volume":"11 2","pages":"71-86"},"PeriodicalIF":0.0,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10232037/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1766114","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/12 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
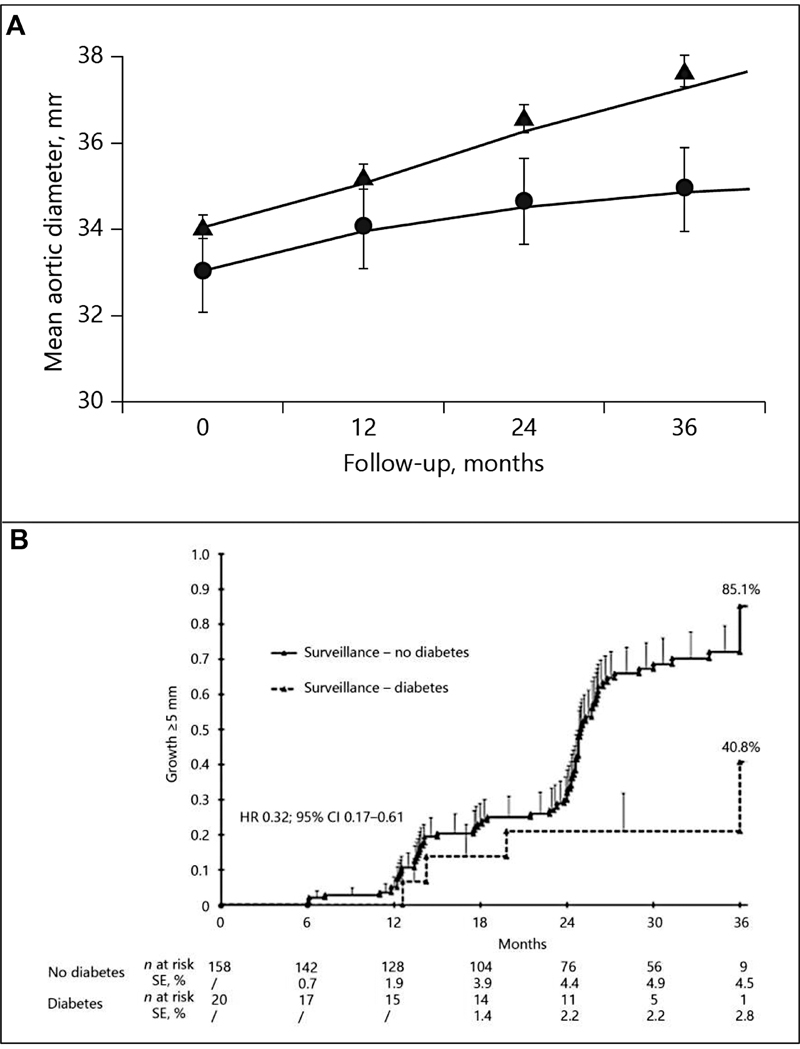
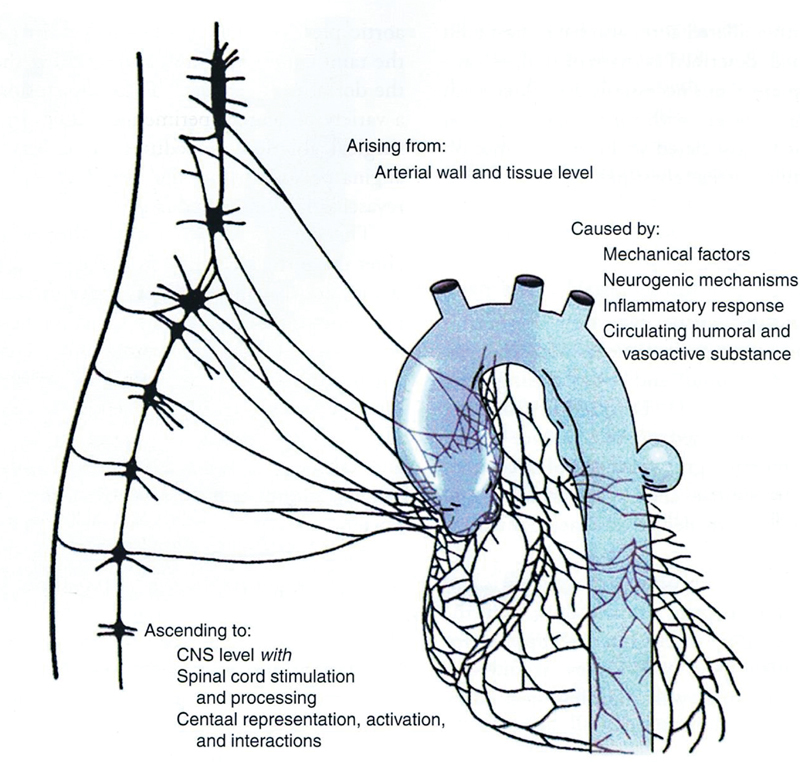
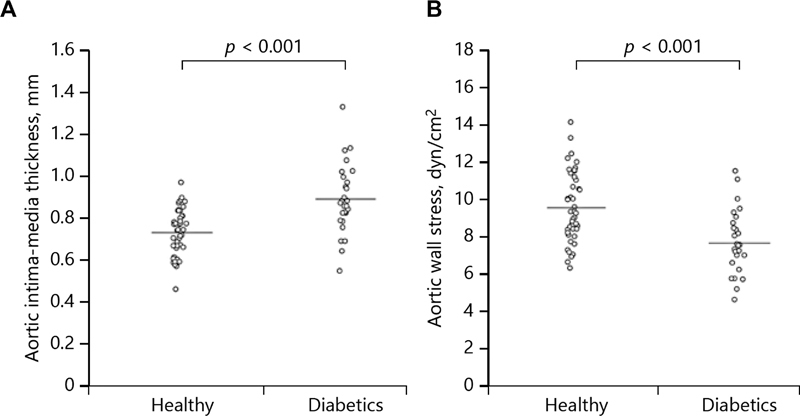
For decades, aortic surgery has relied on size criteria for intervention on the ascending aorta. While diameter has served well, diameter alone falls short of an ideal criterion. Herein, we examine the potential application of other, nondiameter criteria in aortic decision-making. These findings are summarized in this review. We have conducted multiple investigations of specific alternate nonsize criteria by leveraging our extensive database, which includes complete, verified anatomic, clinical, and mortality data on 2,501 patients with thoracic aortic aneurysm (TAA) and dissections (198 Type A, 201 Type B, and 2102 TAAs). We examined 14 potential intervention criteria. Each substudy had its own specific methodology, reported individually in the literature. The overall findings of these studies are presented here, with a special emphasis on how the findings can be incorporated into enhanced aortic decision-making-above and beyond sheer diameter. The following nondiameter criteria have been found useful in decision-making regarding surgical intervention. (1) Pain: In the absence of other specific cause, substernal chest pain mandates surgery. Well-developed afferent neural pathways carry warning signals to the brain. (2) Aortic length/tortuosity: Length is emerging as a mildly better predictor of impending events than diameter. (3) Genes: Specific genetic aberrations provide a powerful predictor of aortic behavior; malignant genetic variants obligate earlier surgery. (4) Family history: Aortic events closely follow those in relatives with a threefold increase in likelihood of aortic dissection for other family members once an index family dissection has occurred. (5) Bicuspid aortic valve: Previously thought to increase aortic risk (as a "Marfan light" situation), current data show that bicuspid valve is not a predictor of higher risk. (6) Diabetes actually protects against aortic events, via mural thickening and fibrosis. (7) Biomarkers: A specialized "RNA signature test" identifies aneurysm-bearing patients in the general population and promises to predict impending dissection. (8) Aortic stress: Blood pressure (BP) elevation from anxiety/exertion precipitates dissection, especially with high-intensity weightlifting. (9) Root dilatation imposes higher dissection risk than supracoronary ascending aneurysm. (10) Inflammation on positron emission tomography (PET) imaging implies high rupture risk and merits surgical intervention. (11) A KIF6 p.Trp719Arg variant elevates aortic dissection risk nearly two-fold. (12) Female sex confers some increased risk, which can be largely accommodated by using body-size-based nomograms (especially height nomograms). (13) Fluoroquinolones predispose to catastrophic dissection events and should be avoided rigorously in aneurysm patients. (14) Advancing age makes the aorta more vulnerable, increasing likelihood of dissection. In conclusion, nondiameter criteria can beneficially be brought to bear on the decision to observe or operate on specific TAA.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
