Daniel J Taylor, Jeroen Feher, Krzysztof Czechowicz, Ian Halliday, D R Hose, Rebecca Gosling, Louise Aubiniere-Robb, Marcel Van't Veer, Danielle C J Keulards, Pim Tonino, Michel Rochette, Julian P Gunn, Paul D Morris
{"title":"Validation of a novel numerical model to predict regionalized blood flow in the coronary arteries.","authors":"Daniel J Taylor, Jeroen Feher, Krzysztof Czechowicz, Ian Halliday, D R Hose, Rebecca Gosling, Louise Aubiniere-Robb, Marcel Van't Veer, Danielle C J Keulards, Pim Tonino, Michel Rochette, Julian P Gunn, Paul D Morris","doi":"10.1093/ehjdh/ztac077","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Ischaemic heart disease results from insufficient coronary blood flow. Direct measurement of absolute flow (mL/min) is feasible, but has not entered routine clinical practice in most catheterization laboratories. Interventional cardiologists, therefore, rely on surrogate markers of flow. Recently, we described a computational fluid dynamics (CFD) method for predicting flow that differentiates inlet, side branch, and outlet flows during angiography. In the current study, we evaluate a new method that regionalizes flow along the length of the artery.</p><p><strong>Methods and results: </strong>Three-dimensional coronary anatomy was reconstructed from angiograms from 20 patients with chronic coronary syndrome. All flows were computed using CFD by applying the pressure gradient to the reconstructed geometry. Side branch flow was modelled as a porous wall boundary. Side branch flow magnitude was based on morphometric scaling laws with two models: a homogeneous model with flow loss along the entire arterial length; and a regionalized model with flow proportional to local taper. Flow results were validated against invasive measurements of flow by continuous infusion thermodilution (Coroventis™, Abbott). Both methods quantified flow relative to the invasive measures: homogeneous (<i>r</i> 0.47, <i>P</i> 0.006; zero bias; 95% CI -168 to +168 mL/min); regionalized method (<i>r</i> 0.43, <i>P</i> 0.013; zero bias; 95% CI -175 to +175 mL/min).</p><p><strong>Conclusion: </strong>During angiography and pressure wire assessment, coronary flow can now be regionalized and differentiated at the inlet, outlet, and side branches. The effect of epicardial disease on agreement suggests the model may be best targeted at cases with a stenosis close to side branches.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"4 2","pages":"81-89"},"PeriodicalIF":4.4000,"publicationDate":"2023-01-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10039427/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztac077","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Ischaemic heart disease results from insufficient coronary blood flow. Direct measurement of absolute flow (mL/min) is feasible, but has not entered routine clinical practice in most catheterization laboratories. Interventional cardiologists, therefore, rely on surrogate markers of flow. Recently, we described a computational fluid dynamics (CFD) method for predicting flow that differentiates inlet, side branch, and outlet flows during angiography. In the current study, we evaluate a new method that regionalizes flow along the length of the artery.
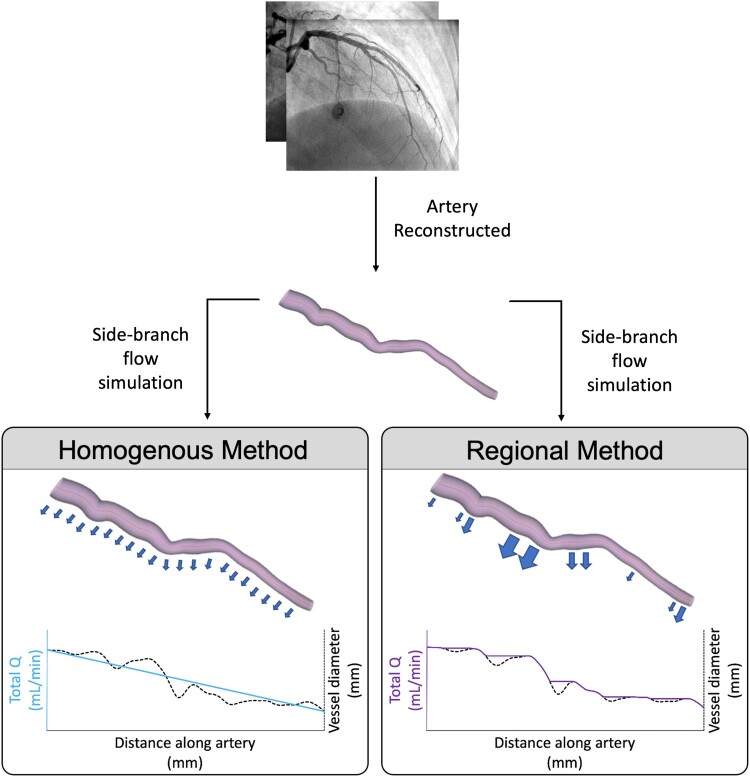
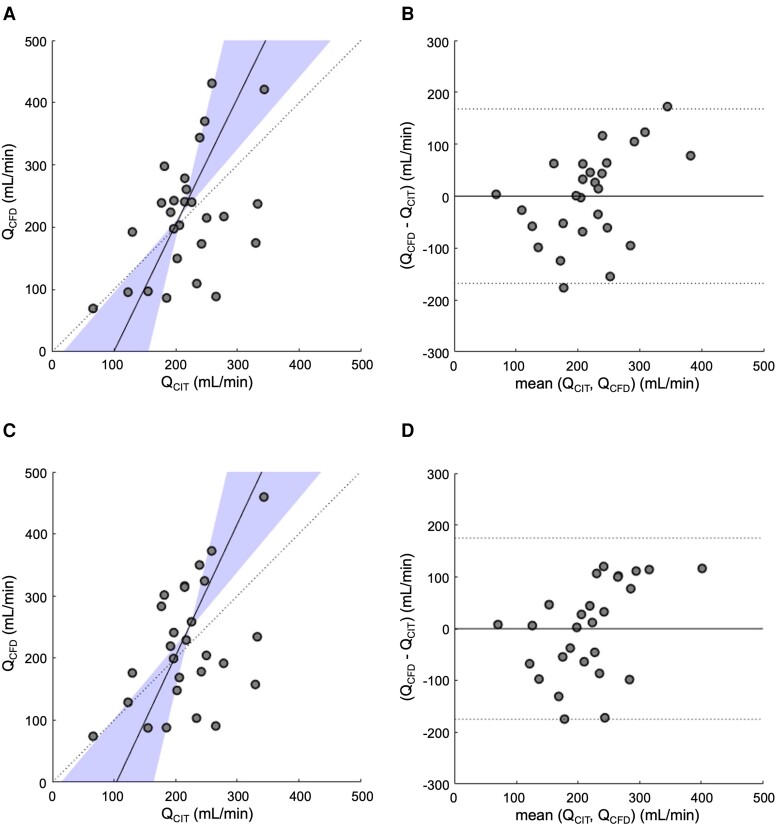
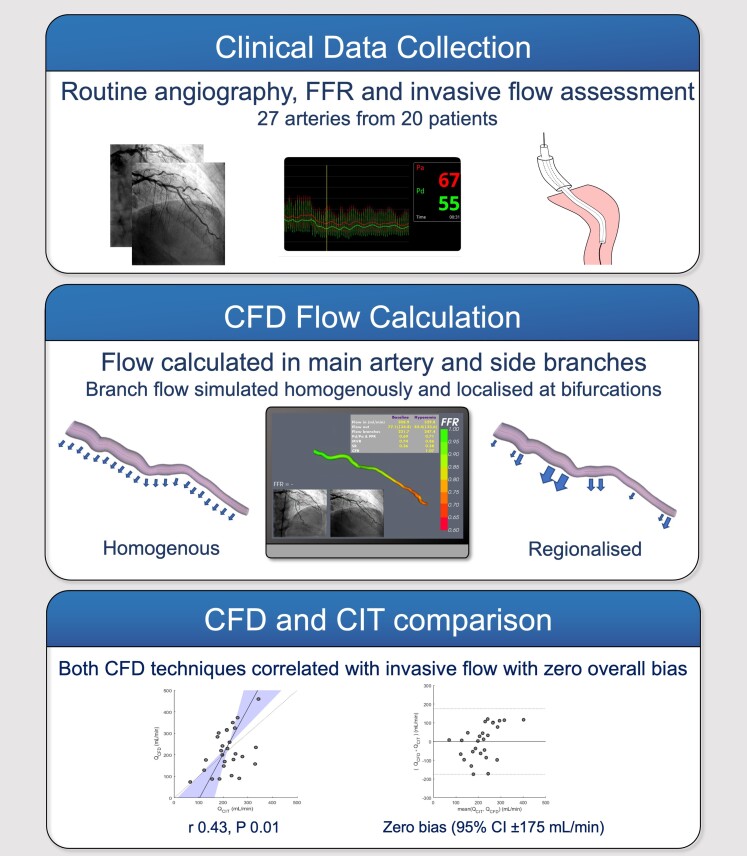
Methods and results: Three-dimensional coronary anatomy was reconstructed from angiograms from 20 patients with chronic coronary syndrome. All flows were computed using CFD by applying the pressure gradient to the reconstructed geometry. Side branch flow was modelled as a porous wall boundary. Side branch flow magnitude was based on morphometric scaling laws with two models: a homogeneous model with flow loss along the entire arterial length; and a regionalized model with flow proportional to local taper. Flow results were validated against invasive measurements of flow by continuous infusion thermodilution (Coroventis™, Abbott). Both methods quantified flow relative to the invasive measures: homogeneous (r 0.47, P 0.006; zero bias; 95% CI -168 to +168 mL/min); regionalized method (r 0.43, P 0.013; zero bias; 95% CI -175 to +175 mL/min).
Conclusion: During angiography and pressure wire assessment, coronary flow can now be regionalized and differentiated at the inlet, outlet, and side branches. The effect of epicardial disease on agreement suggests the model may be best targeted at cases with a stenosis close to side branches.
目的:缺血性心脏病是由冠状动脉血流不足引起的。直接测量绝对流量(mL/min)是可行的,但在大多数导管实验室尚未进入常规临床实践。因此,介入心脏病专家依赖于血流的替代标记物。最近,我们描述了一种计算流体动力学(CFD)方法,用于在血管造影期间区分入口、侧分支和出口流动。在目前的研究中,我们评估了一种新的方法,沿着动脉的长度来划分血流。方法与结果:对20例慢性冠状动脉综合征患者的血管造影资料进行冠状动脉三维解剖重建。通过将压力梯度应用于重建的几何形状,使用CFD计算所有流动。侧枝流动模拟为多孔壁面边界。侧支流量大小基于形态学标度规律,有两种模型:沿整个动脉长度的流量损失均匀模型;建立了流量与局部锥度成正比的区域化模型。通过连续输注热稀释(Coroventis™,雅培)进行有创性流量测量,验证流量结果。两种方法都量化了相对于侵入性措施的流量:均质性(r 0.47, P 0.006;零偏差;95% CI -168 ~ +168 mL/min);区域化方法(r 0.43, P 0.013;零偏差;95% CI -175 ~ +175 mL/min)。结论:在血管造影和压力线评估中,冠状动脉血流可以在入口、出口和侧支进行分区和区分。心外膜疾病对一致性的影响表明该模型可能最适合侧支狭窄的病例。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
