A clinician-to-clinician universal electronic consultation programme at the cardiology department of a Galician healthcare area improves healthcare accessibility and outcomes in elderly patients.
Pilar Mazón-Ramos, Sergio Cinza-Sanjurjo, David Garcia-Vega, Manuel Portela-Romero, Juan C Sanmartin-Pena, Daniel Rey-Aldana, Amparo Martinez-Monzonis, Jenifer Espasandín-Domínguez, Francisco Gude-Sampedro, José R González-Juanatey
{"title":"A clinician-to-clinician universal electronic consultation programme at the cardiology department of a Galician healthcare area improves healthcare accessibility and outcomes in elderly patients.","authors":"Pilar Mazón-Ramos, Sergio Cinza-Sanjurjo, David Garcia-Vega, Manuel Portela-Romero, Juan C Sanmartin-Pena, Daniel Rey-Aldana, Amparo Martinez-Monzonis, Jenifer Espasandín-Domínguez, Francisco Gude-Sampedro, José R González-Juanatey","doi":"10.1093/ehjdh/ztad004","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>We aimed to assess longer-term results (accessibility, hospital admissions, and mortality) in elderly patients referred to a cardiology department (CD) from primary care using e-consultation in outpatient care.</p><p><strong>Methods and results: </strong>We included 9963 patients >80 years from 1 January 2010 to 31 December 2019. Until 2012, all patients attended an in-person consultation (2010-2012). In 2013, we instituted an e-consult programme (2013-2019) for all primary care referrals to cardiologists that preceded a patient's in-person consultation when considered. We used an interrupted time series (ITS) regression approach to investigate the impact of e-consultation on (i) cardiovascular hospital admissions and mortality. We also analysed (ii) the total number and referral rate (population-adjusted referred rate) in both periods, and (iii) the accessibility was measured as the number of consultations and variation according to the distance from the municipality and reference hospital. During e-consultation, the demand for care increased (12.8 ± 4.3% vs. 25.5 ± 11.1% per 1000 inhabitants, <i>P</i> < 0.001) and referrals from different areas were equalized. After the implementation of e-consultation, we observed that the increase in hospital admissions and mortality were stabilized [incidence rate ratio (iRR): 1.351 (95% CI, 0.787, 2.317), <i>P</i> = 0.874] and [iRR: 1.925 (95% CI: 0.889, 4.168), <i>P</i> = 0.096], respectively. The geographic variabilities in hospital admissions and mortality seen during the in-person consultation were stabilized after e-consultation implementation.</p><p><strong>Conclusions: </strong>Implementation of a clinician-to-clinician e-consultation programme in outpatient care was associated with improved accessibility to cardiology healthcare in elderly patients. After e-consultations were implemented, hospital admissions and mortality were stabilized.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"4 2","pages":"90-98"},"PeriodicalIF":4.4000,"publicationDate":"2023-01-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/1a/ztad004.PMC10039426.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztad004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: We aimed to assess longer-term results (accessibility, hospital admissions, and mortality) in elderly patients referred to a cardiology department (CD) from primary care using e-consultation in outpatient care.
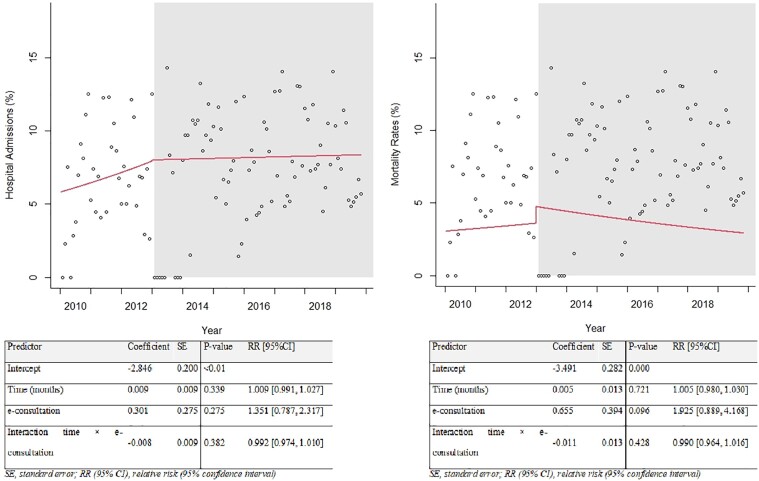
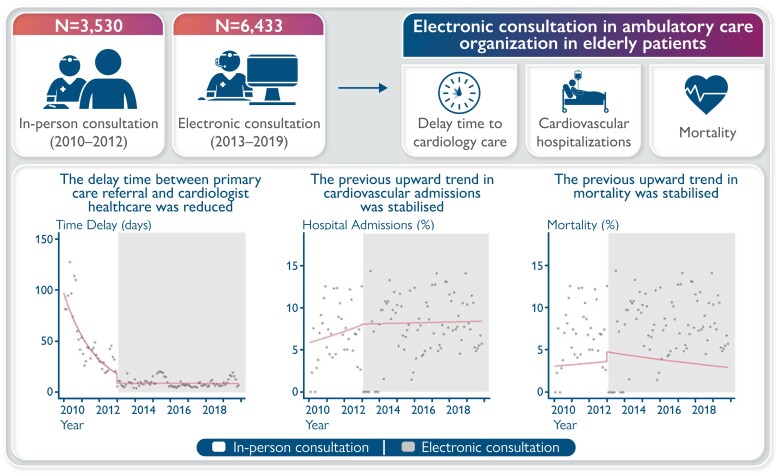
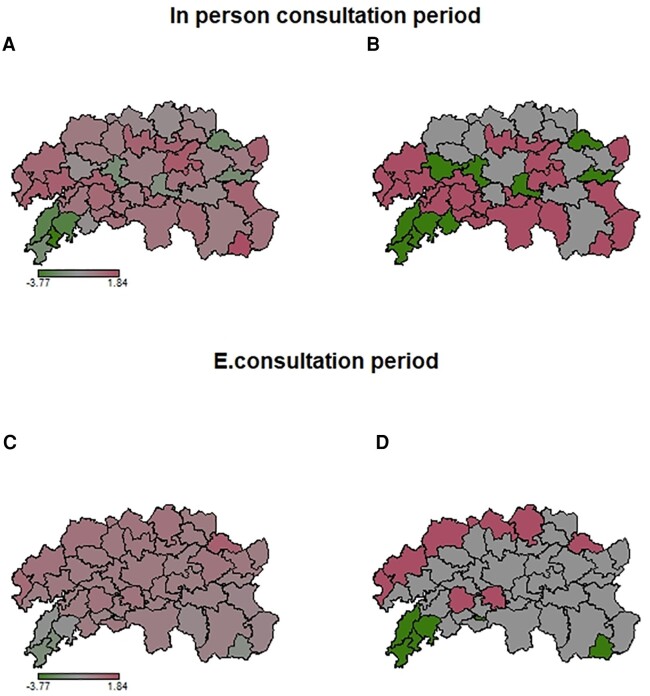
Methods and results: We included 9963 patients >80 years from 1 January 2010 to 31 December 2019. Until 2012, all patients attended an in-person consultation (2010-2012). In 2013, we instituted an e-consult programme (2013-2019) for all primary care referrals to cardiologists that preceded a patient's in-person consultation when considered. We used an interrupted time series (ITS) regression approach to investigate the impact of e-consultation on (i) cardiovascular hospital admissions and mortality. We also analysed (ii) the total number and referral rate (population-adjusted referred rate) in both periods, and (iii) the accessibility was measured as the number of consultations and variation according to the distance from the municipality and reference hospital. During e-consultation, the demand for care increased (12.8 ± 4.3% vs. 25.5 ± 11.1% per 1000 inhabitants, P < 0.001) and referrals from different areas were equalized. After the implementation of e-consultation, we observed that the increase in hospital admissions and mortality were stabilized [incidence rate ratio (iRR): 1.351 (95% CI, 0.787, 2.317), P = 0.874] and [iRR: 1.925 (95% CI: 0.889, 4.168), P = 0.096], respectively. The geographic variabilities in hospital admissions and mortality seen during the in-person consultation were stabilized after e-consultation implementation.
Conclusions: Implementation of a clinician-to-clinician e-consultation programme in outpatient care was associated with improved accessibility to cardiology healthcare in elderly patients. After e-consultations were implemented, hospital admissions and mortality were stabilized.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
