Kris Kumar DO, MSc , Timothy Byrne DO , Timothy F. Simpson MD, PharmD , Ashraf Samhan BS , Raj Shah MD , Jorge Rodriguez MD , Loren Wagner MS , Scott M. Chadderdon MD , Howard K. Song MD, PhD , Harsh Golwala MD , Firas E. Zahr MD
{"title":"Clinical Predictors of Mortality and Heart Failure Hospitalization in Patients With Severe Tricuspid Regurgitation","authors":"Kris Kumar DO, MSc , Timothy Byrne DO , Timothy F. Simpson MD, PharmD , Ashraf Samhan BS , Raj Shah MD , Jorge Rodriguez MD , Loren Wagner MS , Scott M. Chadderdon MD , Howard K. Song MD, PhD , Harsh Golwala MD , Firas E. Zahr MD","doi":"10.1016/j.shj.2022.100130","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>There is an incomplete understanding of the predictors of morbidity and mortality in patients with severe tricuspid regurgitation (TR). This study sought to identify key risk factors for all-cause mortality and heart failure (HF) hospitalization among patients with severe TR.</p></div><div><h3>Methods</h3><p>Patients with severe TR were identified from 2 centers, Oregon Health & Science University and Abrazo Health, from January 01, 2016 to December 31, 2018. Patients with any concomitant severe valvular diseases or prior valvular intervention were excluded. Multivariable regression was utilized to identify demographic, clinical, and echocardiographic variables independently associated with all-cause mortality or HF hospitalization.</p></div><div><h3>Results</h3><p>435 patients with severe TR were followed for a median of 2.8 years. The mean age of the population was 66.9 ± 18.5 years and 58% were female. All-cause mortality was identified in 20.5% of the population. Of the cohort, 35.4% of patients were hospitalized for HF. Isolated tricuspid valve intervention was performed in 2.5% of patients. Independent predictors of all-cause mortality included history of solid tumor (odds ratio [OR] 6.6, 95% confidence interval [CI] 2.1-19.1, <em>p</em> = 0.001), history of peripheral artery disease (OR 3.5, 95% CI 1.2-9.4, <em>p</em> = 0.013), and elevated international normalized ratio in the absence of anticoagulation (OR 1.9, 95% CI 1.2-3.2, <em>p</em> = 0.008). Predictors of HF hospitalization included history of diabetes mellitus (OR 2.2, 95% CI 1.1-4.0, <em>p</em> = 0.014) and history of reduced left ventricular ejection fraction (OR 5.7, 95% CI 2.9-11.7, <em>p</em> < 0.0001).</p></div><div><h3>Conclusions</h3><p>Severe untreated TR is associated with high mortality and frequent HF hospitalizations. Understanding predictors of these outcomes is important to identify patients who may benefit from early tricuspid valve intervention to help improve outcomes in this patient population.</p></div>","PeriodicalId":36053,"journal":{"name":"Structural Heart","volume":"7 2","pages":"Article 100130"},"PeriodicalIF":2.8000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10236773/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Structural Heart","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2474870622019364","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Background
There is an incomplete understanding of the predictors of morbidity and mortality in patients with severe tricuspid regurgitation (TR). This study sought to identify key risk factors for all-cause mortality and heart failure (HF) hospitalization among patients with severe TR.
Methods
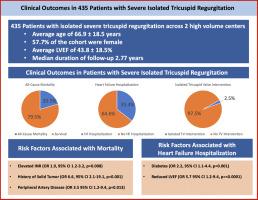
Patients with severe TR were identified from 2 centers, Oregon Health & Science University and Abrazo Health, from January 01, 2016 to December 31, 2018. Patients with any concomitant severe valvular diseases or prior valvular intervention were excluded. Multivariable regression was utilized to identify demographic, clinical, and echocardiographic variables independently associated with all-cause mortality or HF hospitalization.
Results
435 patients with severe TR were followed for a median of 2.8 years. The mean age of the population was 66.9 ± 18.5 years and 58% were female. All-cause mortality was identified in 20.5% of the population. Of the cohort, 35.4% of patients were hospitalized for HF. Isolated tricuspid valve intervention was performed in 2.5% of patients. Independent predictors of all-cause mortality included history of solid tumor (odds ratio [OR] 6.6, 95% confidence interval [CI] 2.1-19.1, p = 0.001), history of peripheral artery disease (OR 3.5, 95% CI 1.2-9.4, p = 0.013), and elevated international normalized ratio in the absence of anticoagulation (OR 1.9, 95% CI 1.2-3.2, p = 0.008). Predictors of HF hospitalization included history of diabetes mellitus (OR 2.2, 95% CI 1.1-4.0, p = 0.014) and history of reduced left ventricular ejection fraction (OR 5.7, 95% CI 2.9-11.7, p < 0.0001).
Conclusions
Severe untreated TR is associated with high mortality and frequent HF hospitalizations. Understanding predictors of these outcomes is important to identify patients who may benefit from early tricuspid valve intervention to help improve outcomes in this patient population.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
