Gideon Leibner, Shuli Brammli-Greenberg, David Katz, Yaakov Esayag, Nechama Kaufman, Adam J Rose
{"title":"Where internal medical patients receive intensive interventions: results from a tertiary-care hospital in Israel.","authors":"Gideon Leibner, Shuli Brammli-Greenberg, David Katz, Yaakov Esayag, Nechama Kaufman, Adam J Rose","doi":"10.1186/s13584-023-00570-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients admitted to internal medicine may be moved to more advanced-care settings when their condition deteriorates. In these advanced care settings, there may be higher levels of monitoring and greater ability to deliver Intensive Medical Treatments (IMTs). To the best of our knowledge, no previous study has examined the proportion of patients at different levels of care who receive different types of IMTs.</p><p><strong>Methods: </strong>In this retrospective observational cohort study, we examined data from 56,002 internal medicine hospitalizations at Shaare Zedek Medical Center, between 01.01.2016 and 31.12.2019. Patients were divided according to where they received care: general-ward, Intermediate-Care Unit, Intensive Care Unit (ICU), or both (Intermediate-Care and ICU). We examined the rates at which these different groups of patients received one or more of the following IMTs: mechanical ventilation, daytime bi-level positive airway pressure (BiPAP), or vasopressor therapy.</p><p><strong>Results: </strong>Most IMTs were delivered in a general-ward setting - ranging from 45.9% of IMT-treated hospitalizations involving combined mechanical ventilation and vasopressor therapy to as high as 87.4% of IMT-treated hospitalizations involving daytime BiPAP. Compared to ICU patients, Intermediate-Care Unit patients were older (mean age 75.1 vs 69.1, p < 0.001 for this and all other comparisons presented here), had longer hospitalizations (21.3 vs 14.5 days), and were more likely to die in-hospital (22% vs 12%). They were also more likely to receive most of the IMTs compared to ICU patients. For example, 9.7% of Intermediate-Care Unit patients received vasopressors, compared to 5.5% of ICU patients.</p><p><strong>Conclusion: </strong>In this study, most of the patients who received IMTs actually received them in a general-bed and not in a dedicated unit. These results imply that IMTs are predominantly delivered in unmonitored settings, and suggest an opportunity to re-examine where and how IMTs are given. In terms of health policy, these findings suggest a need to further examine the setting and patterns of intensive interventions, as well as a need to increase the number of beds dedicated to delivering intensive interventions.</p>","PeriodicalId":46694,"journal":{"name":"Israel Journal of Health Policy Research","volume":"12 1","pages":"22"},"PeriodicalIF":2.2000,"publicationDate":"2023-05-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10206337/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Israel Journal of Health Policy Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13584-023-00570-z","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Patients admitted to internal medicine may be moved to more advanced-care settings when their condition deteriorates. In these advanced care settings, there may be higher levels of monitoring and greater ability to deliver Intensive Medical Treatments (IMTs). To the best of our knowledge, no previous study has examined the proportion of patients at different levels of care who receive different types of IMTs.
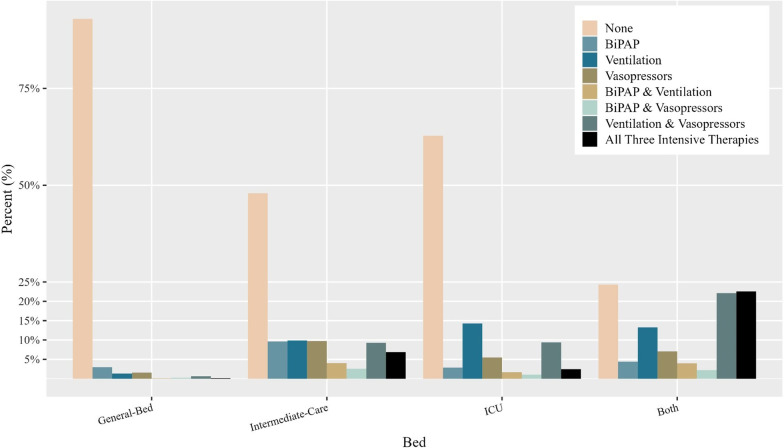
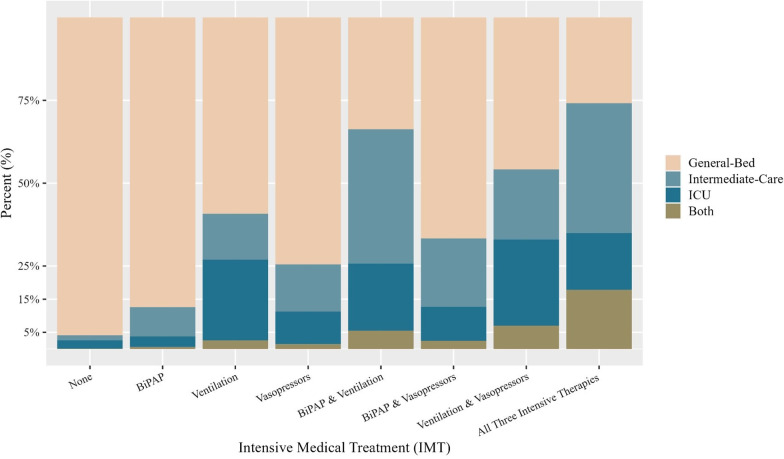
Methods: In this retrospective observational cohort study, we examined data from 56,002 internal medicine hospitalizations at Shaare Zedek Medical Center, between 01.01.2016 and 31.12.2019. Patients were divided according to where they received care: general-ward, Intermediate-Care Unit, Intensive Care Unit (ICU), or both (Intermediate-Care and ICU). We examined the rates at which these different groups of patients received one or more of the following IMTs: mechanical ventilation, daytime bi-level positive airway pressure (BiPAP), or vasopressor therapy.
Results: Most IMTs were delivered in a general-ward setting - ranging from 45.9% of IMT-treated hospitalizations involving combined mechanical ventilation and vasopressor therapy to as high as 87.4% of IMT-treated hospitalizations involving daytime BiPAP. Compared to ICU patients, Intermediate-Care Unit patients were older (mean age 75.1 vs 69.1, p < 0.001 for this and all other comparisons presented here), had longer hospitalizations (21.3 vs 14.5 days), and were more likely to die in-hospital (22% vs 12%). They were also more likely to receive most of the IMTs compared to ICU patients. For example, 9.7% of Intermediate-Care Unit patients received vasopressors, compared to 5.5% of ICU patients.
Conclusion: In this study, most of the patients who received IMTs actually received them in a general-bed and not in a dedicated unit. These results imply that IMTs are predominantly delivered in unmonitored settings, and suggest an opportunity to re-examine where and how IMTs are given. In terms of health policy, these findings suggest a need to further examine the setting and patterns of intensive interventions, as well as a need to increase the number of beds dedicated to delivering intensive interventions.
背景:入住内科的患者在病情恶化时可能会转移到更高级的护理机构。在这些高级护理环境中,可能会有更高水平的监测和更强的能力来提供强化医疗(IMTs)。据我们所知,之前没有研究调查过不同护理水平的患者接受不同类型imt的比例。方法:在这项回顾性观察队列研究中,我们分析了2016年1月1日至2019年12月31日期间Shaare Zedek医疗中心56,002例内科住院患者的数据。患者根据接受护理的地点进行分组:普通病房、中级护理病房、重症监护病房(ICU)或两者兼而有之(中级护理和ICU)。我们检查了这些不同组的患者接受以下一种或多种imt的比率:机械通气、日间双水平气道正压通气(BiPAP)或血管加压治疗。结果:大多数imt是在普通病房进行的,从45.9%的imt治疗住院,包括机械通气和血管加压治疗,到高达87.4%的imt治疗住院,包括日间BiPAP。与ICU患者相比,中间护理病房患者年龄较大(平均年龄75.1 vs 69.1, p)。结论:在本研究中,大多数接受IMTs的患者实际上是在普通病房接受的,而不是在专门的病房接受的。这些结果表明,imt主要是在不受监测的环境中提供的,这表明有机会重新审查在哪里以及如何提供imt。在卫生政策方面,这些调查结果表明,需要进一步审查强化干预措施的环境和模式,并需要增加专门用于提供强化干预措施的床位数量。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
