Kenro Chikazawa, Ken Imai, Masahiro Misawa, Tomoyuki Kuwata
{"title":"A Safe and Standardized Strategy for Laparoscopic Hysterectomy in Patients with a History of Cesarean Section.","authors":"Kenro Chikazawa, Ken Imai, Masahiro Misawa, Tomoyuki Kuwata","doi":"10.4103/gmit.gmit_80_22","DOIUrl":null,"url":null,"abstract":"1. Dissecting the ureter, ligating the cut round ligament, posterior layer of the broad ligament, uterosacral ligament, and infundibulopelvic ligament/ligamentum ovarii proprium 2. Dissection under the bladder pillar bilaterally, followed by dissection under the bladder caudal to the adhesion from the cesarean section 3. If we could not dissect the bladder using step 2, it implied that the adhesions were widespread and we thus would perform dissection more caudally. Therefore, we ligated the uterine artery and the ureteric branches of the uterine artery and dissected the ureter laterally. To reach the vesicouterine pouch from a more caudal and dorsal direction, a dissection under the layer of the uterine artery and superior vesical artery was performed.[3,4] In other words, we reached the vesicouterine pouch under the ureteric tunnel, as is the case during uterine cancer surgery.[5] Thereafter, we approached an area which was more caudal to the adhesion area. This area is usually dissected in a modified radical hysterectomy.","PeriodicalId":45272,"journal":{"name":"Gynecology and Minimally Invasive Therapy-GMIT","volume":"12 1","pages":"46-47"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3e/e5/GMIT-12-46.PMC10071868.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecology and Minimally Invasive Therapy-GMIT","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/gmit.gmit_80_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
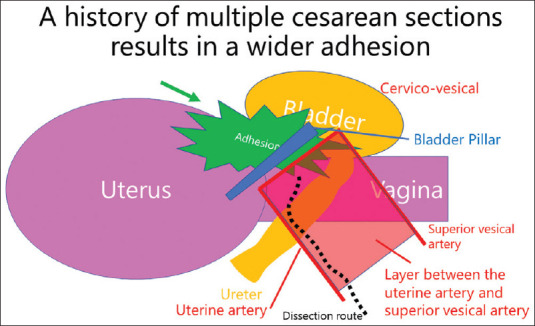
1. Dissecting the ureter, ligating the cut round ligament, posterior layer of the broad ligament, uterosacral ligament, and infundibulopelvic ligament/ligamentum ovarii proprium 2. Dissection under the bladder pillar bilaterally, followed by dissection under the bladder caudal to the adhesion from the cesarean section 3. If we could not dissect the bladder using step 2, it implied that the adhesions were widespread and we thus would perform dissection more caudally. Therefore, we ligated the uterine artery and the ureteric branches of the uterine artery and dissected the ureter laterally. To reach the vesicouterine pouch from a more caudal and dorsal direction, a dissection under the layer of the uterine artery and superior vesical artery was performed.[3,4] In other words, we reached the vesicouterine pouch under the ureteric tunnel, as is the case during uterine cancer surgery.[5] Thereafter, we approached an area which was more caudal to the adhesion area. This area is usually dissected in a modified radical hysterectomy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
