Lingli Zhou, Yingying Luo, Yan Wang, Yao Cheng, Rui Zhang, Simin Zhang, Siqian Gong, Xueyao Han, Linong Ji
{"title":"The clinical implications of fasting serum insulin levels in patients with insulin-treated type 2 diabetes: a cross-sectional survey.","authors":"Lingli Zhou, Yingying Luo, Yan Wang, Yao Cheng, Rui Zhang, Simin Zhang, Siqian Gong, Xueyao Han, Linong Ji","doi":"10.3389/fcdhc.2023.1172208","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to investigate the clinical implications of fasting serum insulin (FINS) levels in subjects with type 2 diabetes who were receiving insulin therapy.</p><p><strong>Methods: </strong>A total of 1,553 subjects with type 2 diabetes [774 subjects who had never received insulin treatment (N-INS) and 779 subjects who were receiving insulin therapy (constant insulin treatment, C-INS)] admitted to the Department of Endocrinology and Metabolism of Peking University People's Hospital were enrolled in this study. Their FINS levels were measured and those with hyperinsulinemia were identified. The underlying mechanisms of hyperinsulinemia were revealed by measuring insulin antibodies (IAs) and analyzing changes in FINS levels before and after polyethylene glycol (PEG) precipitation. In addition, the clinical characteristics of patients with different types of hyperinsulinemia were compared.</p><p><strong>Results: </strong>Higher FINS levels and a higher incidence (43.8%, 341/779) of hyperinsulinemia (FINS > 15μIU/mL) were observed in subjects with C-INS than in subjects with N-INS. Among subjects with C-INS and hyperinsulinemia, 66.9% (228/341) were IAs positive, and the incidence of IAs was found to be positively associated with FINS level. By performing PEG precipitation, we found that all subjects without IAs (i.e., those with real hyperinsulinemia) and 31.1% of subjects (71/228) with IAs (i.e., those with both real and IAs-related hyperinsulinemia) still had hyperinsulinemia after PEG precipitation, whereas FINS levels in the other 68.9% of subjects (157/228) with IAs were normal (IAs-related hyperinsulinemia) after PEG precipitation. Comparisons between the groups showed that subjects with real hyperinsulinemia showed more obvious insulin resistance characteristics, including higher lipid levels, BMIs, and homoeostasis model assessment2-estimated insulin resistance (HOMA2-IR) index, and were more likely to have hypertension, obesity, and metabolic syndromes (<i>p</i> < 0.05). However, the risk of hypoglycemia and glucose variability increased significantly in subjects with IAs compared with those without IAs. A cutoff of FINS to serum C-peptide ratio (≥ 9.3μIU/ng) could be used to screen IAs in clinical practice with 83.3% sensitivity and 70% specificity.</p><p><strong>Conclusions: </strong>It is necessary to measure FINS in subjects with C-INS to distinguish between types of hyperinsulinemia, which should help to tailor treatment regimens.</p>","PeriodicalId":73075,"journal":{"name":"Frontiers in clinical diabetes and healthcare","volume":"4 ","pages":"1172208"},"PeriodicalIF":2.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10266272/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in clinical diabetes and healthcare","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fcdhc.2023.1172208","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study aimed to investigate the clinical implications of fasting serum insulin (FINS) levels in subjects with type 2 diabetes who were receiving insulin therapy.
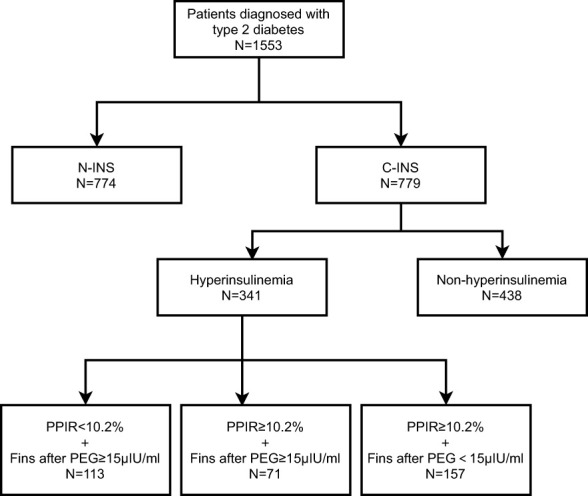
Methods: A total of 1,553 subjects with type 2 diabetes [774 subjects who had never received insulin treatment (N-INS) and 779 subjects who were receiving insulin therapy (constant insulin treatment, C-INS)] admitted to the Department of Endocrinology and Metabolism of Peking University People's Hospital were enrolled in this study. Their FINS levels were measured and those with hyperinsulinemia were identified. The underlying mechanisms of hyperinsulinemia were revealed by measuring insulin antibodies (IAs) and analyzing changes in FINS levels before and after polyethylene glycol (PEG) precipitation. In addition, the clinical characteristics of patients with different types of hyperinsulinemia were compared.
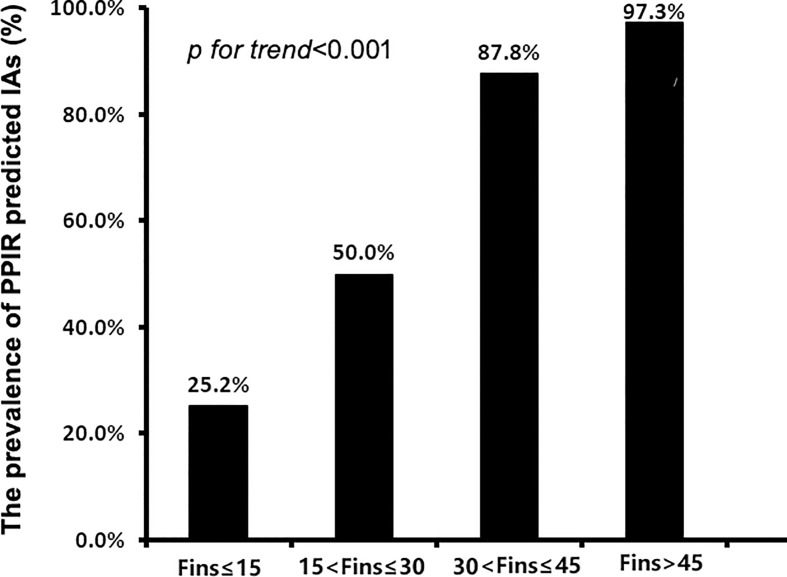
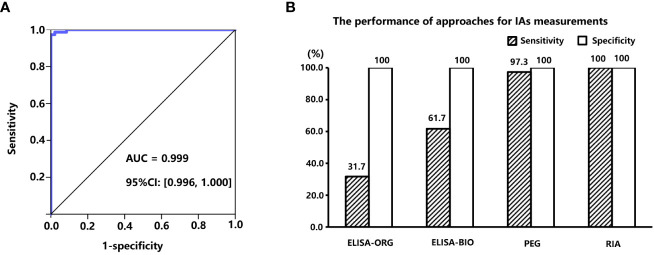
Results: Higher FINS levels and a higher incidence (43.8%, 341/779) of hyperinsulinemia (FINS > 15μIU/mL) were observed in subjects with C-INS than in subjects with N-INS. Among subjects with C-INS and hyperinsulinemia, 66.9% (228/341) were IAs positive, and the incidence of IAs was found to be positively associated with FINS level. By performing PEG precipitation, we found that all subjects without IAs (i.e., those with real hyperinsulinemia) and 31.1% of subjects (71/228) with IAs (i.e., those with both real and IAs-related hyperinsulinemia) still had hyperinsulinemia after PEG precipitation, whereas FINS levels in the other 68.9% of subjects (157/228) with IAs were normal (IAs-related hyperinsulinemia) after PEG precipitation. Comparisons between the groups showed that subjects with real hyperinsulinemia showed more obvious insulin resistance characteristics, including higher lipid levels, BMIs, and homoeostasis model assessment2-estimated insulin resistance (HOMA2-IR) index, and were more likely to have hypertension, obesity, and metabolic syndromes (p < 0.05). However, the risk of hypoglycemia and glucose variability increased significantly in subjects with IAs compared with those without IAs. A cutoff of FINS to serum C-peptide ratio (≥ 9.3μIU/ng) could be used to screen IAs in clinical practice with 83.3% sensitivity and 70% specificity.
Conclusions: It is necessary to measure FINS in subjects with C-INS to distinguish between types of hyperinsulinemia, which should help to tailor treatment regimens.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
