Shelby K Yee, Brenda Y Hernandez, Sandi Kwee, Linda L Wong
{"title":"Hepatocellular carcinoma in Pacific Islanders: comparison of Pacific Island-born <i>vs</i>. US-born.","authors":"Shelby K Yee, Brenda Y Hernandez, Sandi Kwee, Linda L Wong","doi":"10.20517/2394-5079.2022.85","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To describe demographic, clinical, and outcome differences in Pacific Island-born (PI-born) compared to US-born hepatocellular carcinoma (HCC) patients of Pacific Island ancestry within a clinical cohort in Hawaii.</p><p><strong>Methods: </strong>A prospectively collected database of 1608 patients diagnosed with HCC over a 30-year period (1993-2022) identified 252 patients of Pacific Islander ethnicity. Data collected: demographics, medical history, laboratory data, tumor characteristics, treatment, and survival. Patients were divided into two groups: PI-born and US-born. Categorical variables were analyzed using ANOVA and chi-square analysis. Odds ratios with 95% confidence intervals were calculated using univariate and multivariate logistic regression. Overall survival was evaluated using Kaplan-Meier analysis.</p><p><strong>Results: </strong>PI-born patients were younger (57.3 <i>vs</i>. 61.8 years, <i>P</i> = 0.002) and more likely to have hepatitis B (OR 14.10, 7.50-26.50) and underlying cirrhosis (OR 2.28, 1.17-4.45). In comparison, US-born patients had a significantly higher likelihood of Hepatitis C, nonalcoholic steatohepatitis/nonalcoholic fatty liver disease, history of non-HCC cancer, and positive smoking history compared to PI-born patients. PI-born patients were more likely to forego treatment (OR 3.22, 1.77-5.87) and be lost to follow-up (OR 9.21, 1.97-43.03). Both groups were equally likely to have the opportunity for curative surgical treatment (liver resection or transplant). US-born status was associated with higher mortality risk, while transplantation was associated with lower mortality risk. The PI-born cohort demonstrated higher overall survival at 3 and 5 years compared to US-born.</p><p><strong>Conclusion: </strong>HBV remains the primary risk factor for HCC in PI-born patients, whereas HCC in US-born patients is more associated with the adoption of a Westernized lifestyle.</p>","PeriodicalId":12959,"journal":{"name":"Hepatoma Research","volume":"9 ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10079260/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatoma Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.20517/2394-5079.2022.85","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/17 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: To describe demographic, clinical, and outcome differences in Pacific Island-born (PI-born) compared to US-born hepatocellular carcinoma (HCC) patients of Pacific Island ancestry within a clinical cohort in Hawaii.
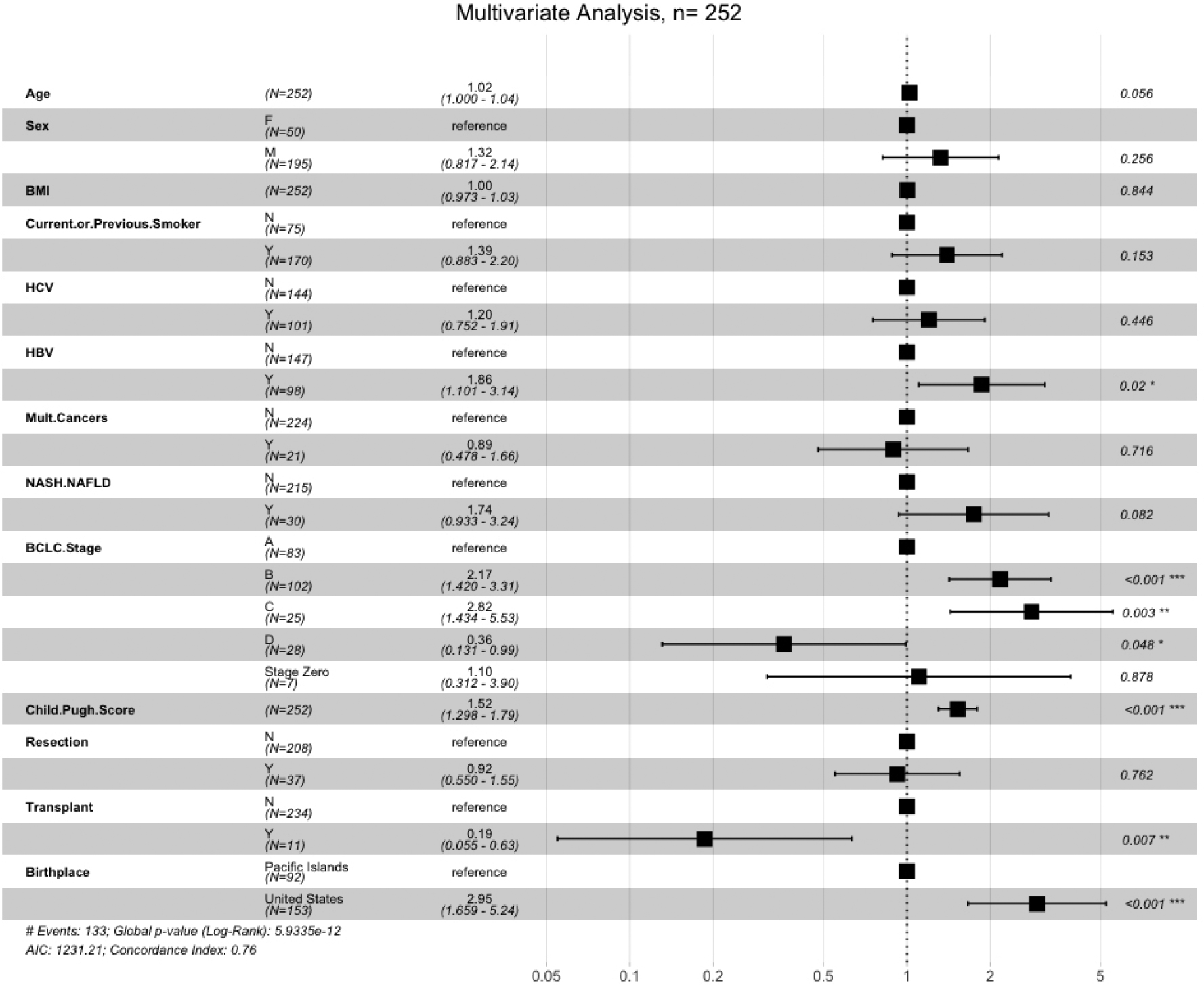
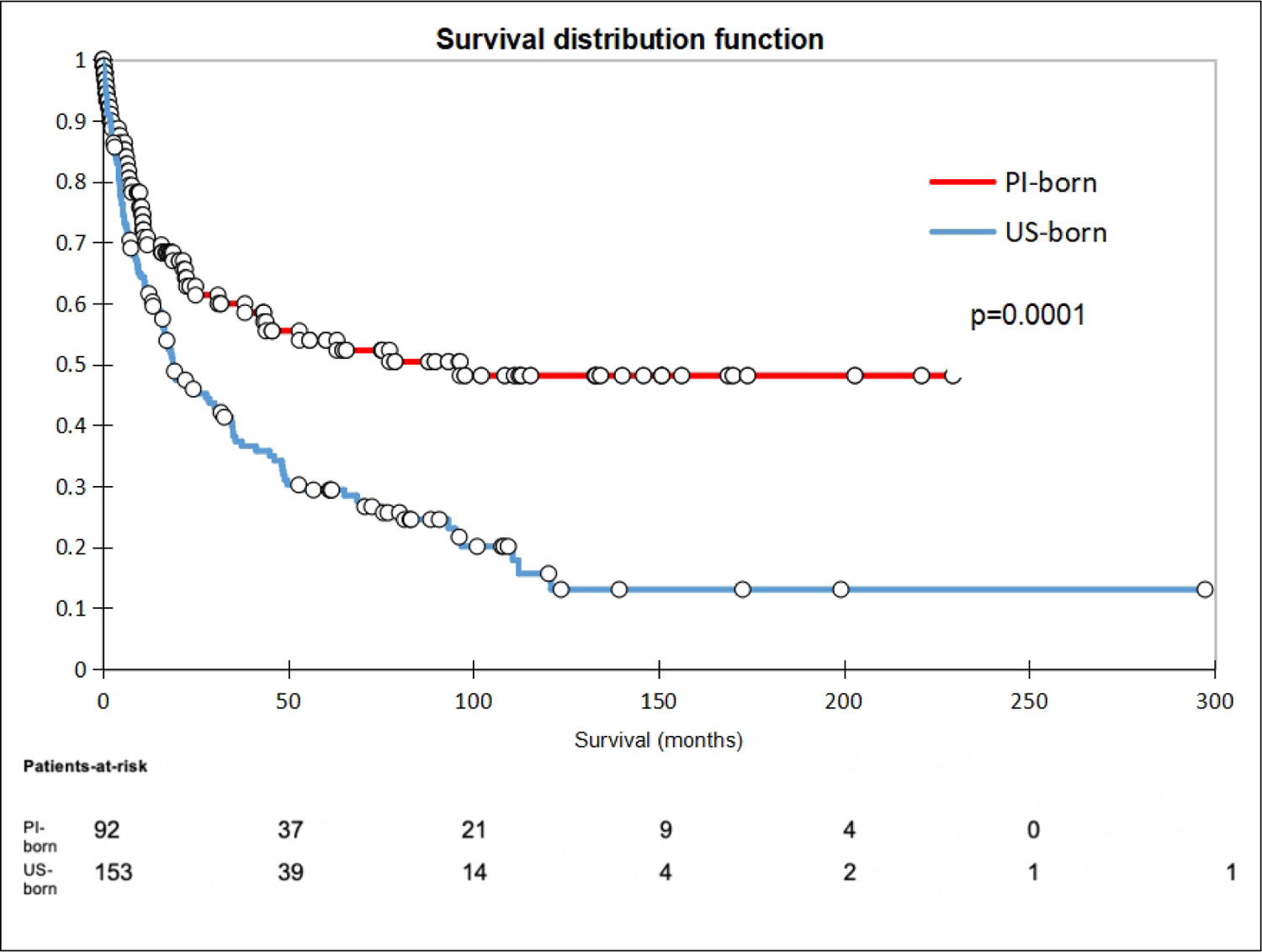
Methods: A prospectively collected database of 1608 patients diagnosed with HCC over a 30-year period (1993-2022) identified 252 patients of Pacific Islander ethnicity. Data collected: demographics, medical history, laboratory data, tumor characteristics, treatment, and survival. Patients were divided into two groups: PI-born and US-born. Categorical variables were analyzed using ANOVA and chi-square analysis. Odds ratios with 95% confidence intervals were calculated using univariate and multivariate logistic regression. Overall survival was evaluated using Kaplan-Meier analysis.
Results: PI-born patients were younger (57.3 vs. 61.8 years, P = 0.002) and more likely to have hepatitis B (OR 14.10, 7.50-26.50) and underlying cirrhosis (OR 2.28, 1.17-4.45). In comparison, US-born patients had a significantly higher likelihood of Hepatitis C, nonalcoholic steatohepatitis/nonalcoholic fatty liver disease, history of non-HCC cancer, and positive smoking history compared to PI-born patients. PI-born patients were more likely to forego treatment (OR 3.22, 1.77-5.87) and be lost to follow-up (OR 9.21, 1.97-43.03). Both groups were equally likely to have the opportunity for curative surgical treatment (liver resection or transplant). US-born status was associated with higher mortality risk, while transplantation was associated with lower mortality risk. The PI-born cohort demonstrated higher overall survival at 3 and 5 years compared to US-born.
Conclusion: HBV remains the primary risk factor for HCC in PI-born patients, whereas HCC in US-born patients is more associated with the adoption of a Westernized lifestyle.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
