A Iyer, Z Ndlovu, J Sharma, H Mansoor, M Bharati, S Kolan, M Morales, M Das, P Issakidis, G Ferlazzo, N Hirani, A Joshi, P Tipre, N Sutar, K England
{"title":"Operationalising targeted next-generation sequencing for routine diagnosis of drug-resistant TB.","authors":"A Iyer, Z Ndlovu, J Sharma, H Mansoor, M Bharati, S Kolan, M Morales, M Das, P Issakidis, G Ferlazzo, N Hirani, A Joshi, P Tipre, N Sutar, K England","doi":"10.5588/pha.22.0041","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Phenotypic drug susceptibility testing (pDST) for <i>Mycobacterium tuberculosis</i> can take up to 8 weeks, while conventional molecular tests identify a limited set of resistance mutations. Targeted next-generation sequencing (tNGS) offers rapid results for predicting comprehensive drug resistance, and this study sought to explore its operational feasibility within a public health laboratory in Mumbai, India.</p><p><strong>Methods: </strong>Pulmonary samples from consenting patients testing Xpert MTB-positive were tested for drug resistance by conventional methods and using tNGS. Laboratory operational and logistical implementation experiences from study team members are shared below.</p><p><strong>Results: </strong>Of the total number of patients tested, 70% (113/161) had no history of previous TB or treatment; however, 88.2% (<i>n</i> = 142) had rifampicin-resistant/multidrug-resistant TB (RR/MDR-TB). There was a high concordance between resistance predictions of tNGS and pDST for most drugs, with tNGS more accurately identifying resistance overall. tNGS was integrated and adapted into the laboratory workflow; however, batching samples caused significantly longer result turnaround time, fastest at 24 days. Manual DNA extraction caused inefficiencies; thus protocol optimisations were performed. Technical expertise was required for analysis of uncharacterised mutations and interpretation of report templates. tNGS cost per sample was US$230, while for pDST this was US$119.</p><p><strong>Conclusions: </strong>Implementation of tNGS is feasible in reference laboratories. It can rapidly identify drug resistance and should be considered as a potential alternative to pDST.</p>","PeriodicalId":46239,"journal":{"name":"Public Health Action","volume":"13 2","pages":"43-49"},"PeriodicalIF":1.6000,"publicationDate":"2023-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10290261/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Public Health Action","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5588/pha.22.0041","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Phenotypic drug susceptibility testing (pDST) for Mycobacterium tuberculosis can take up to 8 weeks, while conventional molecular tests identify a limited set of resistance mutations. Targeted next-generation sequencing (tNGS) offers rapid results for predicting comprehensive drug resistance, and this study sought to explore its operational feasibility within a public health laboratory in Mumbai, India.
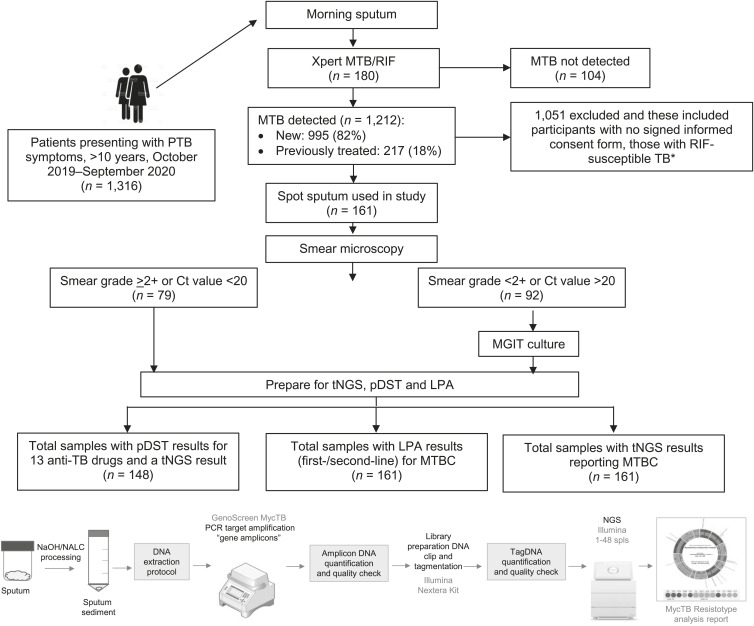
Methods: Pulmonary samples from consenting patients testing Xpert MTB-positive were tested for drug resistance by conventional methods and using tNGS. Laboratory operational and logistical implementation experiences from study team members are shared below.
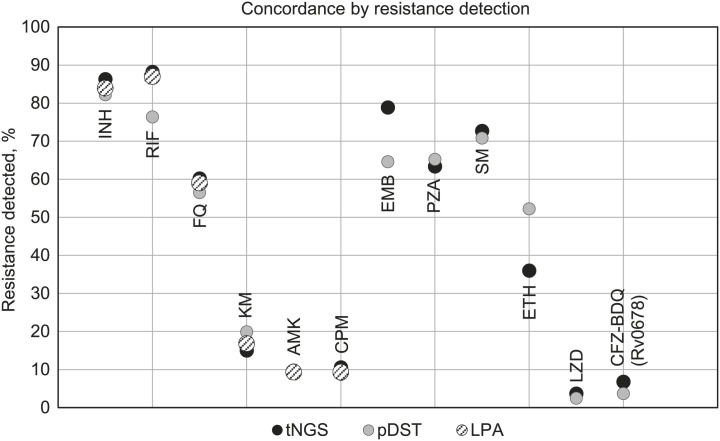
Results: Of the total number of patients tested, 70% (113/161) had no history of previous TB or treatment; however, 88.2% (n = 142) had rifampicin-resistant/multidrug-resistant TB (RR/MDR-TB). There was a high concordance between resistance predictions of tNGS and pDST for most drugs, with tNGS more accurately identifying resistance overall. tNGS was integrated and adapted into the laboratory workflow; however, batching samples caused significantly longer result turnaround time, fastest at 24 days. Manual DNA extraction caused inefficiencies; thus protocol optimisations were performed. Technical expertise was required for analysis of uncharacterised mutations and interpretation of report templates. tNGS cost per sample was US$230, while for pDST this was US$119.
Conclusions: Implementation of tNGS is feasible in reference laboratories. It can rapidly identify drug resistance and should be considered as a potential alternative to pDST.
期刊介绍:
Launched on 1 May 2011, Public Health Action (PHA) is an official publication of the International Union Against Tuberculosis and Lung Disease (The Union). It is an open access, online journal available world-wide to physicians, health workers, researchers, professors, students and decision-makers, including public health centres, medical, university and pharmaceutical libraries, hospitals, clinics, foundations and institutions. PHA is a peer-reviewed scholarly journal that actively encourages, communicates and reports new knowledge, dialogue and controversy in health systems and services for people in vulnerable and resource-limited communities — all topics that reflect the mission of The Union, Health solutions for the poor.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
