{"title":"One Rare Warfarin Resistance Case and Possible Mechanism Exploration.","authors":"Li Zhao, Zhenguo Zhai, Pengmei Li","doi":"10.2147/PGPM.S404474","DOIUrl":null,"url":null,"abstract":"<p><p>One 59-year-old female patient with deep venous thrombosis (DVT) and pulmonary embolism (PE) was treated with 6 mg warfarin once daily as an anticoagulant. Before taking warfarin, her international normalized ratio (INR) was 0.98. Two days after warfarin treatment, her INR did not change from baseline. Due to the high severity of the PE, the patient needed to reach her target range (INR goal = 2.5, range = 2~3) rapidly, so the dose of warfarin was increased from 6 mg daily to 27 mg daily. However, the patient's INR did not improve with the dose escalation, still maintaining an INR of 0.97-0.98. We drew a blood sample half an hour before administering 27 mg warfarin and detected single nucleotide polymorphism for the following genes, which were identified to be relevant with warfarin resistance: CYP2C9 rs1799853, rs1057910, VKORC1 rs9923231, rs61742245, rs7200749, rs55894764, CYP4F2 rs2108622, and GGCX rs2592551. The trough plasma concentration of warfarin was 196.2 ng/mL after 2 days of warfarin administration with 27 mg QD, which was much lower than the therapeutic drug concentration ranges of warfarin (500-3,000 ng/mL). The genotype results demonstrate that the CYP4F2gene has rs2108622 mutation which can explain some aspect of warfarin resistance. Further investigations are necessary to fully characterize other pharmacogenomics or pharmacodynamics determinants of warfarin dose-response in Chinese.</p>","PeriodicalId":56015,"journal":{"name":"Pharmacogenomics & Personalized Medicine","volume":"16 ","pages":"609-615"},"PeriodicalIF":1.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/02/08/pgpm-16-609.PMC10290475.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacogenomics & Personalized Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/PGPM.S404474","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
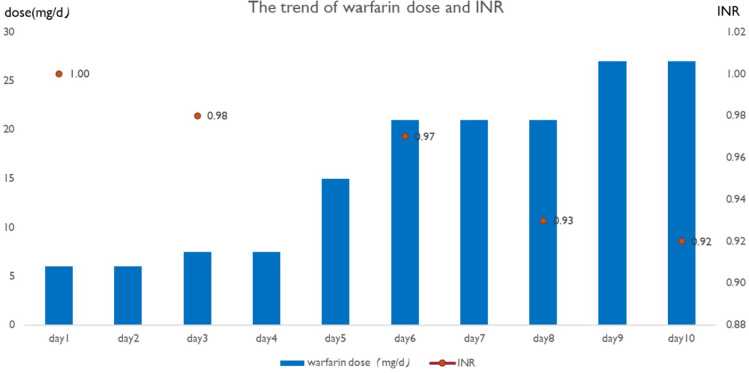
One 59-year-old female patient with deep venous thrombosis (DVT) and pulmonary embolism (PE) was treated with 6 mg warfarin once daily as an anticoagulant. Before taking warfarin, her international normalized ratio (INR) was 0.98. Two days after warfarin treatment, her INR did not change from baseline. Due to the high severity of the PE, the patient needed to reach her target range (INR goal = 2.5, range = 2~3) rapidly, so the dose of warfarin was increased from 6 mg daily to 27 mg daily. However, the patient's INR did not improve with the dose escalation, still maintaining an INR of 0.97-0.98. We drew a blood sample half an hour before administering 27 mg warfarin and detected single nucleotide polymorphism for the following genes, which were identified to be relevant with warfarin resistance: CYP2C9 rs1799853, rs1057910, VKORC1 rs9923231, rs61742245, rs7200749, rs55894764, CYP4F2 rs2108622, and GGCX rs2592551. The trough plasma concentration of warfarin was 196.2 ng/mL after 2 days of warfarin administration with 27 mg QD, which was much lower than the therapeutic drug concentration ranges of warfarin (500-3,000 ng/mL). The genotype results demonstrate that the CYP4F2gene has rs2108622 mutation which can explain some aspect of warfarin resistance. Further investigations are necessary to fully characterize other pharmacogenomics or pharmacodynamics determinants of warfarin dose-response in Chinese.
期刊介绍:
Pharmacogenomics and Personalized Medicine is an international, peer-reviewed, open-access journal characterizing the influence of genotype on pharmacology leading to the development of personalized treatment programs and individualized drug selection for improved safety, efficacy and sustainability.
In particular, emphasis will be given to:
Genomic and proteomic profiling
Genetics and drug metabolism
Targeted drug identification and discovery
Optimizing drug selection & dosage based on patient''s genetic profile
Drug related morbidity & mortality intervention
Advanced disease screening and targeted therapeutic intervention
Genetic based vaccine development
Patient satisfaction and preference
Health economic evaluations
Practical and organizational issues in the development and implementation of personalized medicine programs.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
