{"title":"Intrapapillary capillary loop abundance on nonmagnified blue laser imaging in esophageal intramural pseudodiverticulosis.","authors":"Vincent Zimmer","doi":"10.1097/j.pbj.0000000000000211","DOIUrl":null,"url":null,"abstract":"To the Editor: A 61-year-old male patient with critical alcohol consumption presented with progressive dysphagia and several self-resolved bolus impactions. Index endoscopy indicated a high-grade stricture at 22 cm, warranting passage with a pediatric gastroscope, along with small openings consistent with esophageal intramural pseudodiverticulosis (EIPD). In the distal esophagus, a Schatzki ring emerged with additional pseudodiverticulae. The patient underwent esophageal bougienage to 14 mm. Image-enhanced endoscopy before scheduled repeat bougienage was perfomed, highlighting proximal EIPD on linked color imaging (Fig. 1A). Furthermore, linked color imaging illustrated diffuse spots correlating with what has been designated as the “faux uni” pattern on white light endoscopy. Apart from illustrating active movements with variations of orifice sizes, further characterization using blue laser imaging (BLI) confirmed absent submucosal vessels, while dot-shaped and line-shaped congested intrapapillary capillary loops (IPCL) were clearly appreciated (Fig. 1B). This finding was accentuated in scarred and pseudodiverticula-bearing segments, suggesting EIPD inflammation-driven microvascular alterations (Fig. 1C). Notwithstanding that IPCL changes notably on magnification endoscopy have been reported in other benign esophageal diseases, such as eosinophilic and/or lymphocytic esophagitis (both excluded in this patient), IPCL alterations have never been reported in EIPD nor in any other chronic inflammatory esophageal disorder on nonmagnified conditions (Fig. 1D). Of note, pathology indicating unspecific chronic inflammation did exclude dysplastic changes. While the concept of IPCLs, relying on magnification imageenhanced endoscopy, has been developed to highlight early squamous cell dysplasia and neoplasia, its potential role in chronic inflammatory esophageal diseases awaits further evolution. Albeit not validated for nonenhanced endoscopic assessment, the findings in this patient may suggest IPLC type 2 with uniform dilation and elongation, likewise suggesting a benign condition.","PeriodicalId":74479,"journal":{"name":"Porto biomedical journal","volume":"8 3","pages":"e211"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/06/pj9-8-e211.PMC10289579.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Porto biomedical journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/j.pbj.0000000000000211","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
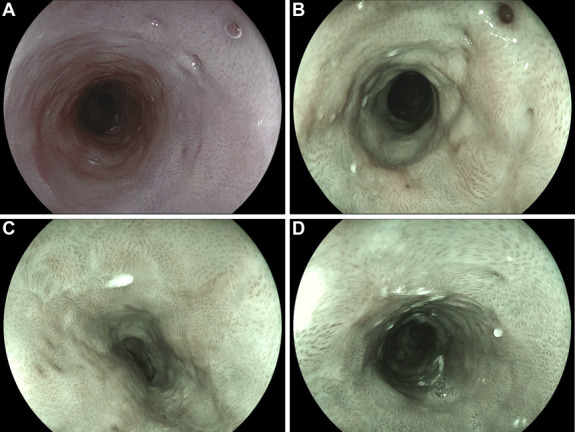
To the Editor: A 61-year-old male patient with critical alcohol consumption presented with progressive dysphagia and several self-resolved bolus impactions. Index endoscopy indicated a high-grade stricture at 22 cm, warranting passage with a pediatric gastroscope, along with small openings consistent with esophageal intramural pseudodiverticulosis (EIPD). In the distal esophagus, a Schatzki ring emerged with additional pseudodiverticulae. The patient underwent esophageal bougienage to 14 mm. Image-enhanced endoscopy before scheduled repeat bougienage was perfomed, highlighting proximal EIPD on linked color imaging (Fig. 1A). Furthermore, linked color imaging illustrated diffuse spots correlating with what has been designated as the “faux uni” pattern on white light endoscopy. Apart from illustrating active movements with variations of orifice sizes, further characterization using blue laser imaging (BLI) confirmed absent submucosal vessels, while dot-shaped and line-shaped congested intrapapillary capillary loops (IPCL) were clearly appreciated (Fig. 1B). This finding was accentuated in scarred and pseudodiverticula-bearing segments, suggesting EIPD inflammation-driven microvascular alterations (Fig. 1C). Notwithstanding that IPCL changes notably on magnification endoscopy have been reported in other benign esophageal diseases, such as eosinophilic and/or lymphocytic esophagitis (both excluded in this patient), IPCL alterations have never been reported in EIPD nor in any other chronic inflammatory esophageal disorder on nonmagnified conditions (Fig. 1D). Of note, pathology indicating unspecific chronic inflammation did exclude dysplastic changes. While the concept of IPCLs, relying on magnification imageenhanced endoscopy, has been developed to highlight early squamous cell dysplasia and neoplasia, its potential role in chronic inflammatory esophageal diseases awaits further evolution. Albeit not validated for nonenhanced endoscopic assessment, the findings in this patient may suggest IPLC type 2 with uniform dilation and elongation, likewise suggesting a benign condition.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
