{"title":"Vancomycin- and piperacillin-induced acute interstitial nephritis in a patient with lupus: A case report showcasing rapid decline in renal function.","authors":"Oluwadamilola Adisa, Anil Ananthaneni, Bryce Rushing, Nathan Rinehouse, Phani Morisetti","doi":"10.5414/CNCS111180","DOIUrl":null,"url":null,"abstract":"<p><p>Drug-induced acute interstitial nephritis (AIN) presents as acute kidney injury (AKI) with the use of certain offending drugs. Antibiotics, such as β-lactams, trimethoprim-sulfamethoxazole, fluoroquinolones, and rifampin, account for up to 50% of drug-induced AIN cases. The onset of drug-induced AIN following drug exposure usually ranges from few days to several weeks or months. We present a patient with lupus who had rapid decline in renal function with a single dose of vancomycin and piperacillin-tazobactam (VPT) administration, termed as the \"workhorse\" regimen at many institutions. In addition, she did not exhibit many clinical and laboratory signs of AIN, making diagnosis challenging. Prompt kidney biopsy and early steroid therapy had a critical role in recovery of the patient's renal function. The median duration for renal impairment in vancomycin-induced AIN is 26 days. Onset of AKI is usually rapid from VPT, within 3 - 5 days of drug exposure. However, the severity of AKI is often low, in contrast to this patient whose AKI reached a stage 3 (AKIN/KDIGO) within 2 days from drug exposure. This study highlights the nephrotoxic potential of piperacillin, especially when used along with vancomycin, concurrent with recent evidence. Within rising antibiotic usage rates, is important to consider AIN in the differential diagnosis of rapidly declining AKI, especially with the combined use of VPT.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"11 ","pages":"99-103"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10286733/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS111180","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
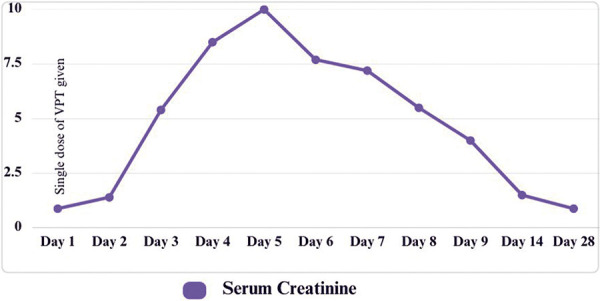
Drug-induced acute interstitial nephritis (AIN) presents as acute kidney injury (AKI) with the use of certain offending drugs. Antibiotics, such as β-lactams, trimethoprim-sulfamethoxazole, fluoroquinolones, and rifampin, account for up to 50% of drug-induced AIN cases. The onset of drug-induced AIN following drug exposure usually ranges from few days to several weeks or months. We present a patient with lupus who had rapid decline in renal function with a single dose of vancomycin and piperacillin-tazobactam (VPT) administration, termed as the "workhorse" regimen at many institutions. In addition, she did not exhibit many clinical and laboratory signs of AIN, making diagnosis challenging. Prompt kidney biopsy and early steroid therapy had a critical role in recovery of the patient's renal function. The median duration for renal impairment in vancomycin-induced AIN is 26 days. Onset of AKI is usually rapid from VPT, within 3 - 5 days of drug exposure. However, the severity of AKI is often low, in contrast to this patient whose AKI reached a stage 3 (AKIN/KDIGO) within 2 days from drug exposure. This study highlights the nephrotoxic potential of piperacillin, especially when used along with vancomycin, concurrent with recent evidence. Within rising antibiotic usage rates, is important to consider AIN in the differential diagnosis of rapidly declining AKI, especially with the combined use of VPT.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
