{"title":"Effect of the Gastrojejunostomy Position on the Postoperative Amount of Oral Intake in Pancreaticoduodenectomy.","authors":"Hiroya Iida, Hiromitsu Maehira, Takeru Maekawa, Haruki Mori, Nobuhito Nitta, Katsushi Takebayashi, Masatsugu Kojima, Mika Kurihara, Shigeki Bamba, Masaya Sasaki, Masaji Tani","doi":"10.1159/000525551","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>We investigated the effect of the gastrojejunostomy position on the postoperative oral intake in patients who have undergone pancreaticoduodenectomy (PD).</p><p><strong>Methods: </strong>We investigated 119 patients who underwent PD between June 2013 and December 2019 and examined the effect of the horizontal and vertical distance rates of the gastrojejunostomy position on the postoperative oral intake. The patients were categorized as having poor or good oral intake based on whether their intake was up to half the required calorie intake.</p><p><strong>Results: </strong>There were significant differences in the number of cases with grade B or C postoperative pancreatic fistula (good, 20.3% vs. poor, 60.0%; p < 0.001), horizontal distance rate (good, 0.57 vs. poor, 0.48; p = 0.02), and postoperative hospitalization period (good, 15 vs. poor, 35 days; p < 0.001). However, there was no significant difference in the vertical distance rate (good, 0.67 vs. poor, 0.71; p = 0.22). The horizontal distance rate was the independent risk factor for postoperative poor oral intake at 2-3 weeks (risk ratio, 3.69; 95% CI: 1.48-9.20).</p><p><strong>Discussion: </strong>The oral intake was greater in patients whose gastrojejunostomy position in PD was farther from the median, suggesting the necessity of intraoperative placement of the gastrojejunostomy position as far from the median as possible.</p>","PeriodicalId":12222,"journal":{"name":"European Surgical Research","volume":"64 2","pages":"211-219"},"PeriodicalIF":1.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10332481/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Surgical Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000525551","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: We investigated the effect of the gastrojejunostomy position on the postoperative oral intake in patients who have undergone pancreaticoduodenectomy (PD).
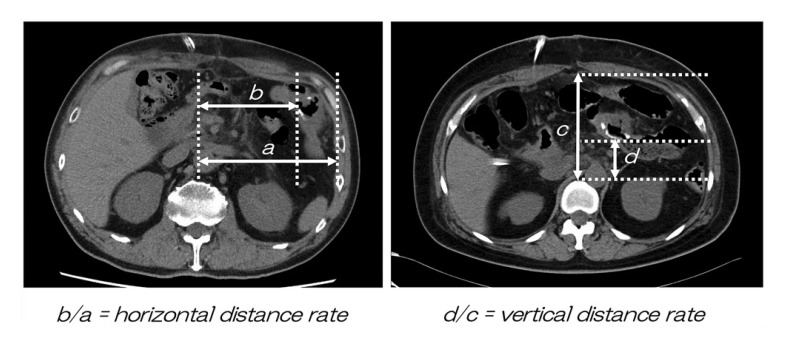
Methods: We investigated 119 patients who underwent PD between June 2013 and December 2019 and examined the effect of the horizontal and vertical distance rates of the gastrojejunostomy position on the postoperative oral intake. The patients were categorized as having poor or good oral intake based on whether their intake was up to half the required calorie intake.
Results: There were significant differences in the number of cases with grade B or C postoperative pancreatic fistula (good, 20.3% vs. poor, 60.0%; p < 0.001), horizontal distance rate (good, 0.57 vs. poor, 0.48; p = 0.02), and postoperative hospitalization period (good, 15 vs. poor, 35 days; p < 0.001). However, there was no significant difference in the vertical distance rate (good, 0.67 vs. poor, 0.71; p = 0.22). The horizontal distance rate was the independent risk factor for postoperative poor oral intake at 2-3 weeks (risk ratio, 3.69; 95% CI: 1.48-9.20).
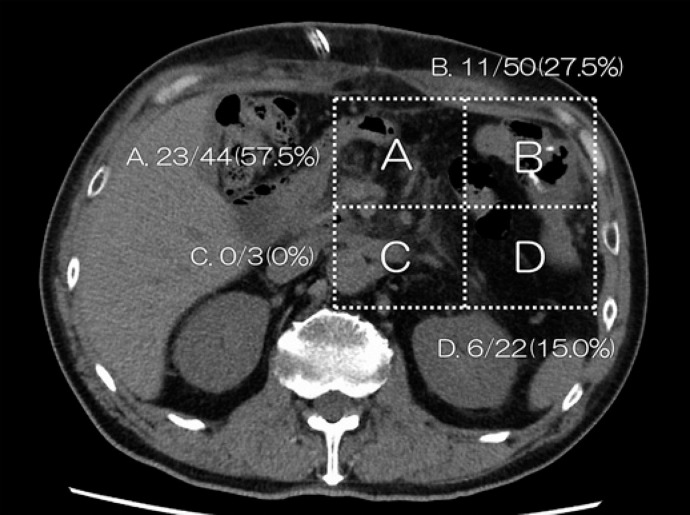
Discussion: The oral intake was greater in patients whose gastrojejunostomy position in PD was farther from the median, suggesting the necessity of intraoperative placement of the gastrojejunostomy position as far from the median as possible.
期刊介绍:
''European Surgical Research'' features original clinical and experimental papers, condensed reviews of new knowledge relevant to surgical research, and short technical notes serving the information needs of investigators in various fields of operative medicine. Coverage includes surgery, surgical pathophysiology, drug usage, and new surgical techniques. Special consideration is given to information on the use of animal models, physiological and biological methods as well as biophysical measuring and recording systems. The journal is of particular value for workers interested in pathophysiologic concepts, new techniques and in how these can be introduced into clinical work or applied when critical decisions are made concerning the use of new procedures or drugs.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
