{"title":"The superdominant RCA with double PDA.","authors":"Mesut Mutluoglu, Kristof De-Smet, Ilse Crevits, Stefaan Gryspeerdt","doi":"10.24875/ACM.21000402","DOIUrl":null,"url":null,"abstract":"*Correspondence: Mesut Mutluoglu E-mail: mesut.mutluoglu@azdelta.be Available online: 02-02-2023 Arch Cardiol Mex. 2023;93(1):105-106 www.archivoscardiologia.com Date of reception: 19-12-2021 Date of acceptance: 15-03-2022 DOI: 10.24875/ACM.21000402 Coronary artery anomalies (CAAs) are congenital disorders observed anywhere along the trajectory of the coronary arteries with an incidence around 0.61.3%1. The right coronary artery (RCA) is dominant in 85% of the general population and supplies the posterior descending artery (PDA) and posterolateral artery (PLA) branches1. The term superdominant has been coined to describe a coronary artery with one or more additional branches which take over the perfusion of a territory that is normally perfused by the other coronary artery which, in this case, is missing one of its main branches1. In this specific case, we have incidentally identified an extremely rare variant of the coronary circulation with an hypoplastic left circumflex artery (LCx) (Fig. 1A red arrow) and a prominent so-called ‘superdominant’ RCA (Fig.1B red arrow) which after delivering a normal interventricular R-PDA (Fig. 1B white arrow) extends leftwards beyond the crux cordis and continues within the atrioventricular sulcus to deliver a second PDA, namely, the R-PLA (Fig. 1B yellow arrow), parallel to the original one, to supply the inferior and posterolateral walls of the left ventricle, normally perfused by the LCx. While several previous studies suggested an increased risk for atherosclerosis in patients with CAA, there is as yet no established consensus on the precise implications of coronary anomalies on the long-term prognosis2. Funding","PeriodicalId":8360,"journal":{"name":"Archivos de cardiologia de Mexico","volume":"93 1","pages":"105-106"},"PeriodicalIF":0.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c1/af/7567AX221-ACM-93-105.PMC10161838.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archivos de cardiologia de Mexico","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24875/ACM.21000402","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
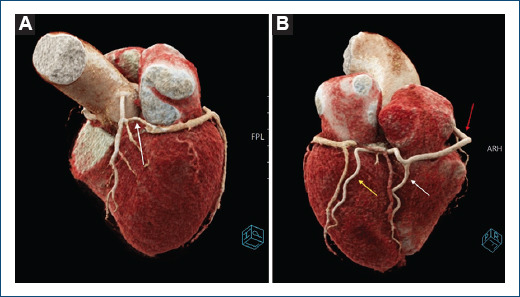
*Correspondence: Mesut Mutluoglu E-mail: mesut.mutluoglu@azdelta.be Available online: 02-02-2023 Arch Cardiol Mex. 2023;93(1):105-106 www.archivoscardiologia.com Date of reception: 19-12-2021 Date of acceptance: 15-03-2022 DOI: 10.24875/ACM.21000402 Coronary artery anomalies (CAAs) are congenital disorders observed anywhere along the trajectory of the coronary arteries with an incidence around 0.61.3%1. The right coronary artery (RCA) is dominant in 85% of the general population and supplies the posterior descending artery (PDA) and posterolateral artery (PLA) branches1. The term superdominant has been coined to describe a coronary artery with one or more additional branches which take over the perfusion of a territory that is normally perfused by the other coronary artery which, in this case, is missing one of its main branches1. In this specific case, we have incidentally identified an extremely rare variant of the coronary circulation with an hypoplastic left circumflex artery (LCx) (Fig. 1A red arrow) and a prominent so-called ‘superdominant’ RCA (Fig.1B red arrow) which after delivering a normal interventricular R-PDA (Fig. 1B white arrow) extends leftwards beyond the crux cordis and continues within the atrioventricular sulcus to deliver a second PDA, namely, the R-PLA (Fig. 1B yellow arrow), parallel to the original one, to supply the inferior and posterolateral walls of the left ventricle, normally perfused by the LCx. While several previous studies suggested an increased risk for atherosclerosis in patients with CAA, there is as yet no established consensus on the precise implications of coronary anomalies on the long-term prognosis2. Funding



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
