Association between left ventricular lead position and intrinsic QRS morphology with regard to clinical outcome in cardiac resynchronization therapy for heart failure
Tove Olsson Brandtvig MSc, Sofia Marinko MD, Maiwand Farouq MD, Johan Brandt MD, PhD, David Mörtsell MD, PhD, Lingwei Wang MD, PhD, Uzma Chaudhry MD, PhD, Samir Saba MD, Rasmus Borgquist MD, PhD
{"title":"Association between left ventricular lead position and intrinsic QRS morphology with regard to clinical outcome in cardiac resynchronization therapy for heart failure","authors":"Tove Olsson Brandtvig MSc, Sofia Marinko MD, Maiwand Farouq MD, Johan Brandt MD, PhD, David Mörtsell MD, PhD, Lingwei Wang MD, PhD, Uzma Chaudhry MD, PhD, Samir Saba MD, Rasmus Borgquist MD, PhD","doi":"10.1111/anec.13065","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Left ventricular (LV) lead position may be an important factor for delivering effective cardiac resynchronization therapy (CRT). We therefore aimed to evaluate the effects of LV lead position, stratified by native QRS morphology, regarding the clinical outcome.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A total of 1295 CRT-implanted patients were retrospectively evaluated. LV lead position was classified as lateral, anterior, inferior, or apical, and was determined using the left and right anterior oblique X-ray views. Kaplan Meier and Cox regression were performed to evaluate the effects on all-cause mortality and heart failure hospitalization, and the potential interaction between LV lead position and native ECG morphologies.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 1295 patients were included. Patients were aged 69 ± 7 years, 20% were female, 46% received a CRT-Pacemaker (vs. CRT-Defibrillator), mean LVEF was 25% ± 7%, and median follow-up was 3.3 years [IQR 1.6–5–7 years]. Eight hundred and eighty-two patients (68%) had a lateral LV lead location, 207 (16%) anterior, 155 (12%) apical, and 51 (4%) inferior. Patients with lateral LV lead position had larger QRS reduction (−13 ± 27 ms vs. −3 ± 24 ms, <i>p</i> < .001). Non-lateral lead location was associated with a higher risk for all-cause mortality (HR 1.34 [1.09–1.67], <i>p</i> = .007) and heart failure hospitalization (HR 1.25 [1.03–1.52], <i>p</i> = .03). This association was strongest for patients with native left or right bundle branch block, and not significant for patients with prior paced QRS or nonspecific intraventricular conduction delay.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>In patients treated with CRT, non-lateral LV lead positions (including apical, anterior, and inferior positions) were associated with worse clinical outcome and less reduction of QRS duration. This association was strongest for patients with native LBBB or RBBB.</p>\n </section>\n </div>","PeriodicalId":8074,"journal":{"name":"Annals of Noninvasive Electrocardiology","volume":"28 4","pages":""},"PeriodicalIF":1.1000,"publicationDate":"2023-05-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/90/b1/ANEC-28-e13065.PMC10335614.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Noninvasive Electrocardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/anec.13065","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Left ventricular (LV) lead position may be an important factor for delivering effective cardiac resynchronization therapy (CRT). We therefore aimed to evaluate the effects of LV lead position, stratified by native QRS morphology, regarding the clinical outcome.
Methods
A total of 1295 CRT-implanted patients were retrospectively evaluated. LV lead position was classified as lateral, anterior, inferior, or apical, and was determined using the left and right anterior oblique X-ray views. Kaplan Meier and Cox regression were performed to evaluate the effects on all-cause mortality and heart failure hospitalization, and the potential interaction between LV lead position and native ECG morphologies.
Results
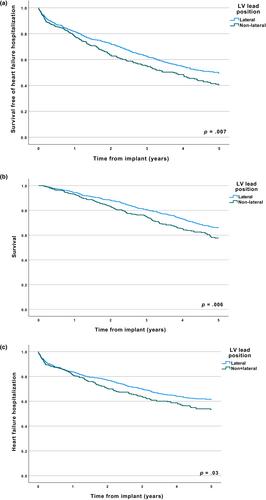
A total of 1295 patients were included. Patients were aged 69 ± 7 years, 20% were female, 46% received a CRT-Pacemaker (vs. CRT-Defibrillator), mean LVEF was 25% ± 7%, and median follow-up was 3.3 years [IQR 1.6–5–7 years]. Eight hundred and eighty-two patients (68%) had a lateral LV lead location, 207 (16%) anterior, 155 (12%) apical, and 51 (4%) inferior. Patients with lateral LV lead position had larger QRS reduction (−13 ± 27 ms vs. −3 ± 24 ms, p < .001). Non-lateral lead location was associated with a higher risk for all-cause mortality (HR 1.34 [1.09–1.67], p = .007) and heart failure hospitalization (HR 1.25 [1.03–1.52], p = .03). This association was strongest for patients with native left or right bundle branch block, and not significant for patients with prior paced QRS or nonspecific intraventricular conduction delay.
Conclusions
In patients treated with CRT, non-lateral LV lead positions (including apical, anterior, and inferior positions) were associated with worse clinical outcome and less reduction of QRS duration. This association was strongest for patients with native LBBB or RBBB.
背景左心室导联位置可能是提供有效心脏再同步化治疗(CRT)的重要因素。因此,我们的目的是评估左室导联位置对临床结果的影响,并按本地QRS形态学分层。方法对1295例ct植入患者进行回顾性分析。左室导联位置分为外侧、前方、下方或顶端,并通过左、右前斜x线片确定。Kaplan Meier和Cox回归评估了对全因死亡率和心力衰竭住院的影响,以及左室导联位置和原生心电图形态之间的潜在相互作用。结果共纳入1295例患者。患者年龄69±7岁,20%为女性,46%接受了crt起搏器(vs. crt除颤器),平均LVEF为25%±7%,中位随访时间为3.3年[IQR为1.6-5-7年]。882例(68%)患者左室导联位于外侧,207例(16%)位于前方,155例(12%)位于顶端,51例(4%)位于下方。左室侧导联患者QRS降低幅度较大(- 13±27 ms vs - 3±24 ms, p < 0.001)。非外侧导联位置与全因死亡率(HR 1.34 [1.09-1.67], p = .007)和心力衰竭住院(HR 1.25 [1.03-1.52], p = .03)相关。这种相关性在原生左束或右束分支阻滞患者中最强,而在既往有节奏性QRS或非特异性脑室传导延迟的患者中不显著。结论在接受CRT治疗的患者中,非侧位左室导联(包括心尖、前位和下位)与较差的临床结果和较短的QRS持续时间相关。这种关联在先天LBBB或RBBB患者中最强。
期刊介绍:
The ANNALS OF NONINVASIVE ELECTROCARDIOLOGY (A.N.E) is an online only journal that incorporates ongoing advances in the clinical application and technology of traditional and new ECG-based techniques in the diagnosis and treatment of cardiac patients.
ANE is the first journal in an evolving subspecialty that incorporates ongoing advances in the clinical application and technology of traditional and new ECG-based techniques in the diagnosis and treatment of cardiac patients. The publication includes topics related to 12-lead, exercise and high-resolution electrocardiography, arrhythmias, ischemia, repolarization phenomena, heart rate variability, circadian rhythms, bioengineering technology, signal-averaged ECGs, T-wave alternans and automatic external defibrillation.
ANE publishes peer-reviewed articles of interest to clinicians and researchers in the field of noninvasive electrocardiology. Original research, clinical studies, state-of-the-art reviews, case reports, technical notes, and letters to the editors will be published to meet future demands in this field.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
