{"title":"Long-term outcomes of surgical aortic valve replacement in patients receiving chronic dialysis.","authors":"Defen Peng, Jamil Bashir, James Abel, Jian Ye","doi":"10.1503/cjs.019121","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgical aortic valve replacement (SAVR) has been the standard treatment for symptomatic severe aortic stenosis, which is common among patients receiving long-term dialysis. The aim of this study was to report the long-term outcomes of SAVR in patients receiving chronic dialysis and to identify independent risk factors for early and late mortality.</p><p><strong>Methods: </strong>Every consecutive patient with SAVR with or without concomitant cardiac procedures in British Columbia between January 2000 and December 2015 was identified from the provincial cardiac registry. The Kaplan-Meier method was used to estimate survival. Univariate and multivariable models were conducted to determine independent risk factors for short-term mortality and reduced long-term survival.</p><p><strong>Results: </strong>Between 2000 and 2015, 654 patients receiving dialysis underwent SAVR with or without concomitant procedures. The mean follow-up was 2.3 (standard deviation 2.4) years (median 2.5 yr). The overall 30-day mortality was 12.8%. The 5-year and 10-year survival rates were 45.6% and 23.5%, respectively. Twelve patients (1.8%) had redo aortic valve surgery. There was no difference in 30-day mortality or long-term survival between 2 age groups (> 65 yr v. ≤ 65 yr). Anemia and cardiopulmonary bypass (CPB) were independent risk factors for both longer hospital stay and reduced long-term survival. The impact of CPB pump time on mortality occurred mainly within the first 30 days after surgery. When CPB pump time extended beyond 170 minutes, there was a significant increase in 30-day mortality with further prolongation of CPB pump time, and the relationship between 30-day mortality and CPB pump time became approximately linear.</p><p><strong>Conclusion: </strong>Patients receiving dialysis have poor long-term survival with a very low rate of redo aortic valve surgery following SAVR with or without concomitant procedures. Older age (> 65 yr) is not an independent risk factor for either 30-day mortality or reduced long-term survival. Using alternative strategies to limit CPB pump time is an important way to reduce 30-day mortality.</p>","PeriodicalId":9573,"journal":{"name":"Canadian Journal of Surgery","volume":"66 4","pages":"E358-E366"},"PeriodicalIF":2.2000,"publicationDate":"2023-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/05/b7/066E358.PMC10322159.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cjs.019121","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Surgical aortic valve replacement (SAVR) has been the standard treatment for symptomatic severe aortic stenosis, which is common among patients receiving long-term dialysis. The aim of this study was to report the long-term outcomes of SAVR in patients receiving chronic dialysis and to identify independent risk factors for early and late mortality.
Methods: Every consecutive patient with SAVR with or without concomitant cardiac procedures in British Columbia between January 2000 and December 2015 was identified from the provincial cardiac registry. The Kaplan-Meier method was used to estimate survival. Univariate and multivariable models were conducted to determine independent risk factors for short-term mortality and reduced long-term survival.
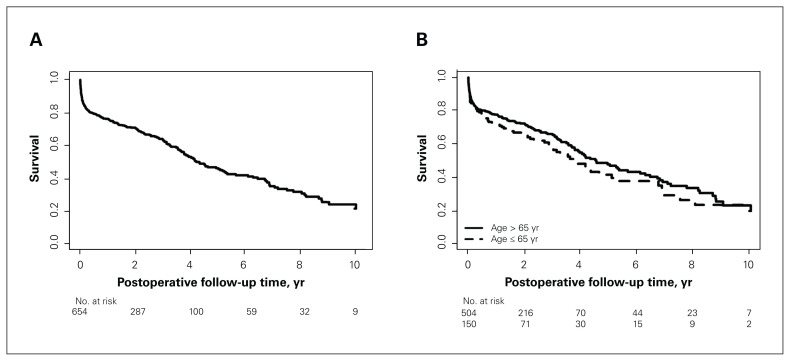
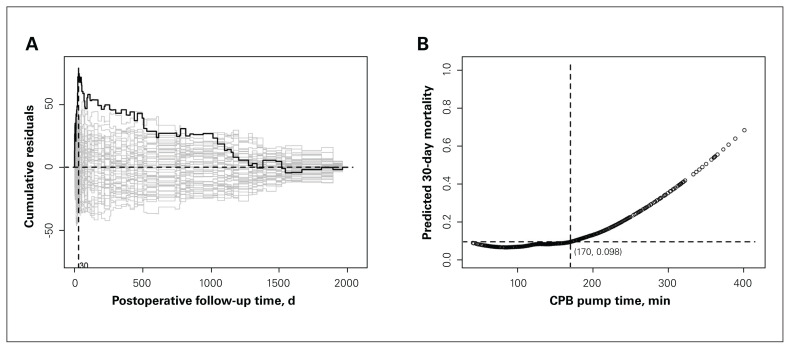
Results: Between 2000 and 2015, 654 patients receiving dialysis underwent SAVR with or without concomitant procedures. The mean follow-up was 2.3 (standard deviation 2.4) years (median 2.5 yr). The overall 30-day mortality was 12.8%. The 5-year and 10-year survival rates were 45.6% and 23.5%, respectively. Twelve patients (1.8%) had redo aortic valve surgery. There was no difference in 30-day mortality or long-term survival between 2 age groups (> 65 yr v. ≤ 65 yr). Anemia and cardiopulmonary bypass (CPB) were independent risk factors for both longer hospital stay and reduced long-term survival. The impact of CPB pump time on mortality occurred mainly within the first 30 days after surgery. When CPB pump time extended beyond 170 minutes, there was a significant increase in 30-day mortality with further prolongation of CPB pump time, and the relationship between 30-day mortality and CPB pump time became approximately linear.
Conclusion: Patients receiving dialysis have poor long-term survival with a very low rate of redo aortic valve surgery following SAVR with or without concomitant procedures. Older age (> 65 yr) is not an independent risk factor for either 30-day mortality or reduced long-term survival. Using alternative strategies to limit CPB pump time is an important way to reduce 30-day mortality.
期刊介绍:
The mission of CJS is to contribute to the meaningful continuing medical education of Canadian surgical specialists, and to provide surgeons with an effective vehicle for the dissemination of observations in the areas of clinical and basic science research.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
