Sonya Burgess, Craig P Juergens, Wesley Yang, Ibrahim M Shugman, Hanan Idris, Tuan Nguyen, Alison McLean, Sarah Zaman, Liza Thomas, Kristy P Robledo, Christian Mussap, Sidney Lo, John French
{"title":"Sex Differences in Outcome and Prescribing Practice in ST-elevation MI Patients with Multivessel Disease and Incomplete Revascularisation.","authors":"Sonya Burgess, Craig P Juergens, Wesley Yang, Ibrahim M Shugman, Hanan Idris, Tuan Nguyen, Alison McLean, Sarah Zaman, Liza Thomas, Kristy P Robledo, Christian Mussap, Sidney Lo, John French","doi":"10.15420/ecr.2022.39","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective:</b> To investigate the extent to which multivessel disease, incomplete revascularisation and prescribing differences contribute to sex-based outcome disparities in patients with ST-elevation MI (STEMI) and establish whether differences in cardiac death and MI (CDMI) rates persist at long-term follow-up. <b>Methods and results:</b> This observational study evaluates sex-based outcome differences (median follow-up 3.6 years; IQR [2.4-5.4]) in a consecutive cohort of patients (n=2,083) presenting with STEMI undergoing percutaneous coronary intervention). Of the studied patients 20.3% (423/2,083) were women and 38.3% (810/2,083) had multivessel disease (MVD). Incomplete revascularisation was common. The median residual SYNTAX score (rSS) was 5.0 (IQR [0-9]) in women and 5.0 (IQR [1-11]) in men (p=0.369), and in patients with MVD it was 9 (IQR [6-17]) in women and 10 (IQR [6-15]) in men (p=0.838). The primary endpoint CDMI occurred in 20.3% of women (86/423) and in 13.2% of men (219/1,660) (p=0.028). Differences persisted following multivariable risk adjustment: female sex was independently associated with CDMI (aHR 1.33; IQR [1.02-1.74]). Women with MVD had CDMI more often than all other groups (p<0.001 for all). Significant sex-based prescribing differences were evident: women were less likely to receive guideline-recommended potent P2Y12 inhibitors than men (31% versus 43%; p=0.012), and differences were particularly evident in patients with MVD (25% in women versus 45% in men, p=0.011). <b>Conclusion</b>: Sex-based differences in STEMI patient outcome persist at long-term follow-up. Poor outcomes were disproportionately found in women with MVD and those with rSS>8. Observed differences in P2Y<sub>12</sub> prescribing practices may contribute to poor outcomes for women with MVD and incomplete revascularisation.</p>","PeriodicalId":45957,"journal":{"name":"European Cardiology Review","volume":"18 ","pages":"e10"},"PeriodicalIF":3.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/df/a0/ecr-18-e10.PMC10316337.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Cardiology Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/ecr.2022.39","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
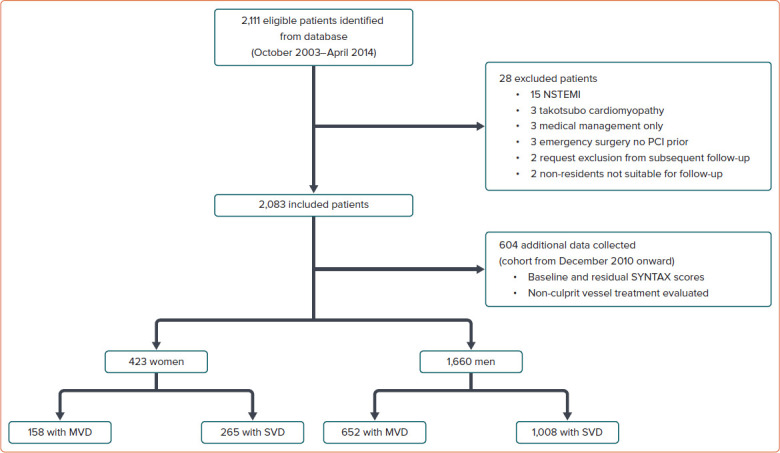
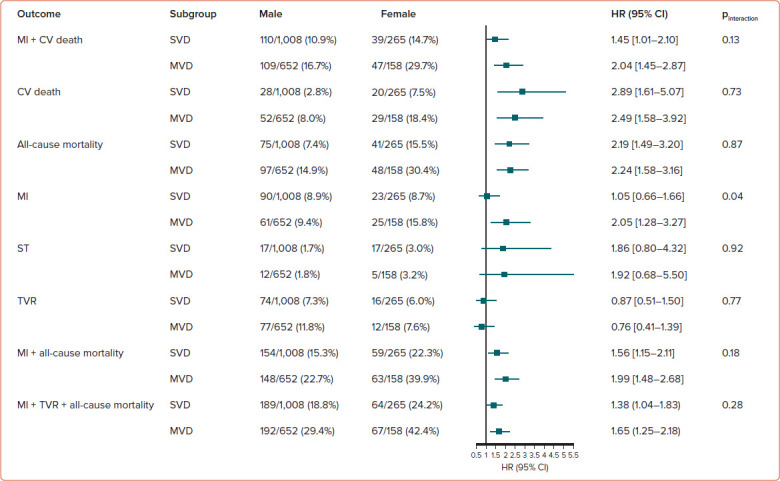
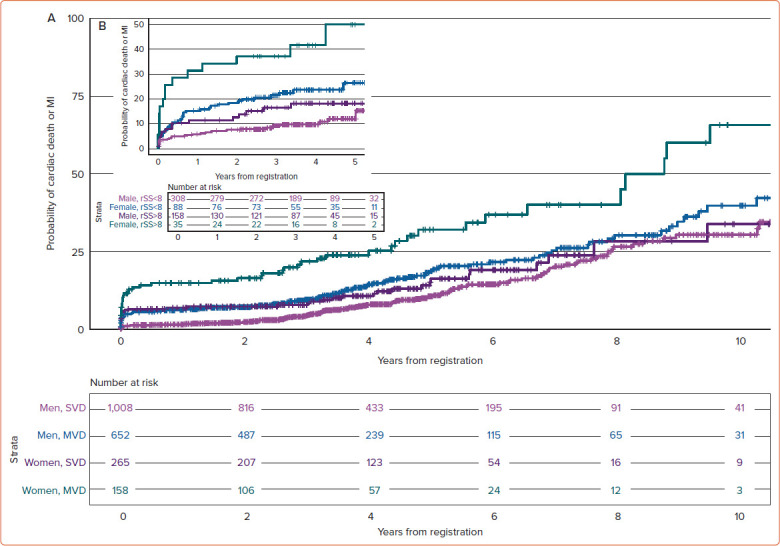
Objective: To investigate the extent to which multivessel disease, incomplete revascularisation and prescribing differences contribute to sex-based outcome disparities in patients with ST-elevation MI (STEMI) and establish whether differences in cardiac death and MI (CDMI) rates persist at long-term follow-up. Methods and results: This observational study evaluates sex-based outcome differences (median follow-up 3.6 years; IQR [2.4-5.4]) in a consecutive cohort of patients (n=2,083) presenting with STEMI undergoing percutaneous coronary intervention). Of the studied patients 20.3% (423/2,083) were women and 38.3% (810/2,083) had multivessel disease (MVD). Incomplete revascularisation was common. The median residual SYNTAX score (rSS) was 5.0 (IQR [0-9]) in women and 5.0 (IQR [1-11]) in men (p=0.369), and in patients with MVD it was 9 (IQR [6-17]) in women and 10 (IQR [6-15]) in men (p=0.838). The primary endpoint CDMI occurred in 20.3% of women (86/423) and in 13.2% of men (219/1,660) (p=0.028). Differences persisted following multivariable risk adjustment: female sex was independently associated with CDMI (aHR 1.33; IQR [1.02-1.74]). Women with MVD had CDMI more often than all other groups (p<0.001 for all). Significant sex-based prescribing differences were evident: women were less likely to receive guideline-recommended potent P2Y12 inhibitors than men (31% versus 43%; p=0.012), and differences were particularly evident in patients with MVD (25% in women versus 45% in men, p=0.011). Conclusion: Sex-based differences in STEMI patient outcome persist at long-term follow-up. Poor outcomes were disproportionately found in women with MVD and those with rSS>8. Observed differences in P2Y12 prescribing practices may contribute to poor outcomes for women with MVD and incomplete revascularisation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
