Performance of the Enhanced Liver Fibrosis Score, Comparison with Vibration-controlled Transient Elastography Data, and Development of a Simple Algorithm to Predict Significant Liver Fibrosis in a Community-based Liver Service: A Retrospective Evaluation.
Tina Reinson, Janisha Patel, Mead Mathews, Derek Fountain, Ryan M Buchanan, Christopher D Byrne
{"title":"Performance of the Enhanced Liver Fibrosis Score, Comparison with Vibration-controlled Transient Elastography Data, and Development of a Simple Algorithm to Predict Significant Liver Fibrosis in a Community-based Liver Service: A Retrospective Evaluation.","authors":"Tina Reinson, Janisha Patel, Mead Mathews, Derek Fountain, Ryan M Buchanan, Christopher D Byrne","doi":"10.14218/JCTH.2022.00335","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Liver fibrosis is a key risk factor for cirrhosis, hepatocellular carcinoma and end stage liver failure. The National Institute for Health and Care Excellence guidelines for assessment for advanced (≥F3) liver fibrosis in people with nonalcoholic fatty liver disease recommend the use of enhanced liver fibrosis (ELF) test, followed by vibration-controlled transient elastography (VCTE). Performance of ELF at predicting significant (≥F2) fibrosis in real-world practice is uncertain. To assess the accuracy of ELF using VCTE; investigate the optimum ELF cutoff value to identify ≥F2 and ≥F3; and develop a simple algorithm, with and without ELF score, for detecting ≥F2.</p><p><strong>Methods: </strong>Retrospective evaluation of patients referred to a Community Liver Service for VCTE, Jan-Dec 2020. Assessment included: body mass index (BMI), diabetes status, alanine aminotransferase (ALT) levels, ELF score and biopsy-validated fibrosis stages according to VCTE.</p><p><strong>Results: </strong>Data from 273 patients were available. <i>n</i>=110 patients had diabetes. ELF showed fair performance for ≥F2 and ≥F3, area under the curve (AUC) = 0.70, 95% confidence interval (CI) 0.64-0.76 and AUC=0.72, 95% CI: 0.65-0.79 respectively. For ≥F2 Youden's index for ELF=9.85 and for ≥F3, ELF=9.95. Combining ALT, BMI, and HbA1c (ALBA algorithm) to predict ≥F2 showed good performance (AUC=0.80, 95% CI: 0.69-0.92), adding ALBA to ELF improved performance (AUC=0.82, 95% CI: 0.77-0.88). Results were independently validated.</p><p><strong>Conclusions: </strong>Optimal ELF cutoff for ≥F2 is 9.85 and 9.95 for ≥F3. ALT, BMI, and HbA1c (ALBA algorithm) can stratify patients at risk of ≥F2. ELF performance is improved by adding ALBA.</p>","PeriodicalId":15484,"journal":{"name":"Journal of Clinical and Translational Hepatology","volume":"11 4","pages":"800-808"},"PeriodicalIF":4.2000,"publicationDate":"2023-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a5/7f/JCTH-11-800.PMC10318295.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Translational Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14218/JCTH.2022.00335","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
Background and aims: Liver fibrosis is a key risk factor for cirrhosis, hepatocellular carcinoma and end stage liver failure. The National Institute for Health and Care Excellence guidelines for assessment for advanced (≥F3) liver fibrosis in people with nonalcoholic fatty liver disease recommend the use of enhanced liver fibrosis (ELF) test, followed by vibration-controlled transient elastography (VCTE). Performance of ELF at predicting significant (≥F2) fibrosis in real-world practice is uncertain. To assess the accuracy of ELF using VCTE; investigate the optimum ELF cutoff value to identify ≥F2 and ≥F3; and develop a simple algorithm, with and without ELF score, for detecting ≥F2.
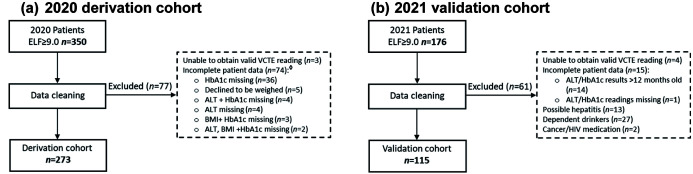
Methods: Retrospective evaluation of patients referred to a Community Liver Service for VCTE, Jan-Dec 2020. Assessment included: body mass index (BMI), diabetes status, alanine aminotransferase (ALT) levels, ELF score and biopsy-validated fibrosis stages according to VCTE.
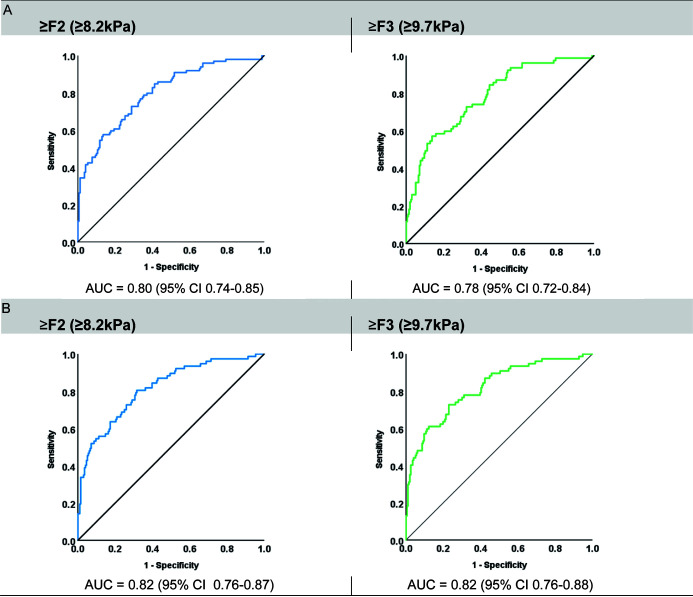
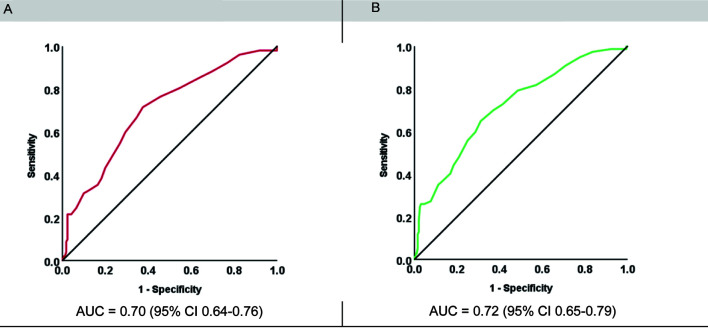
Results: Data from 273 patients were available. n=110 patients had diabetes. ELF showed fair performance for ≥F2 and ≥F3, area under the curve (AUC) = 0.70, 95% confidence interval (CI) 0.64-0.76 and AUC=0.72, 95% CI: 0.65-0.79 respectively. For ≥F2 Youden's index for ELF=9.85 and for ≥F3, ELF=9.95. Combining ALT, BMI, and HbA1c (ALBA algorithm) to predict ≥F2 showed good performance (AUC=0.80, 95% CI: 0.69-0.92), adding ALBA to ELF improved performance (AUC=0.82, 95% CI: 0.77-0.88). Results were independently validated.
Conclusions: Optimal ELF cutoff for ≥F2 is 9.85 and 9.95 for ≥F3. ALT, BMI, and HbA1c (ALBA algorithm) can stratify patients at risk of ≥F2. ELF performance is improved by adding ALBA.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
