Nuria Ginjaume Garcia, Cristina Soler Moreno, Natalia Teixeira, Pia Español Lloret, Rocío Luna Guibourg, Ramon Rovira Negre
{"title":"Comparison of Laparoscopy and Laparotomy in the Management of Early-stage Ovarian Cancer.","authors":"Nuria Ginjaume Garcia, Cristina Soler Moreno, Natalia Teixeira, Pia Español Lloret, Rocío Luna Guibourg, Ramon Rovira Negre","doi":"10.4103/gmit.gmit_99_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The objective of this study was to assess the feasibility of minimally invasive surgery for early-stage ovarian cancer (EOC) by comparing the surgical and survival outcomes between laparoscopy and laparotomy.</p><p><strong>Materials and methods: </strong>This was a retrospective, single-center observational study that included all patients who underwent surgical staging for EOC by laparoscopy or laparotomy between 2010 and 2019.</p><p><strong>Results: </strong>Forty-nine patients were included; of which 20 underwent laparoscopy, 26 laparotomy, and three conversion from laparoscopy to laparotomy. No significant differences were observed between the two groups regarding operative time, number of lymph nodes dissected, or intraoperative tumor rupture rate, while estimated blood loss and transfusion requirements were lower in the laparoscopy group. The complication rate tended to be higher in the laparotomy group. Patients in the laparoscopy group had a faster recovery, with earlier urinary catheter and abdominal drain removal, shorter hospital stay, and a trend toward earlier tolerance of oral diet and mobilization. At a mean follow-up of 45.7 months, 14 patients had disease recurrence, with no differences in the mean progression-free survival between the two groups (36 months for laparoscopy vs. 35.5 months for laparotomy, <i>P</i> = 0.22).</p><p><strong>Conclusion: </strong>Laparoscopic surgery performed by a trained gynecological oncologist is a safe and effective surgical approach for comprehensive staging of EOC, with the additional benefits of a faster recovery compared to laparotomy.</p>","PeriodicalId":45272,"journal":{"name":"Gynecology and Minimally Invasive Therapy-GMIT","volume":"12 2","pages":"83-89"},"PeriodicalIF":1.7000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a1/1c/GMIT-12-83.PMC10321349.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecology and Minimally Invasive Therapy-GMIT","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/gmit.gmit_99_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: The objective of this study was to assess the feasibility of minimally invasive surgery for early-stage ovarian cancer (EOC) by comparing the surgical and survival outcomes between laparoscopy and laparotomy.
Materials and methods: This was a retrospective, single-center observational study that included all patients who underwent surgical staging for EOC by laparoscopy or laparotomy between 2010 and 2019.
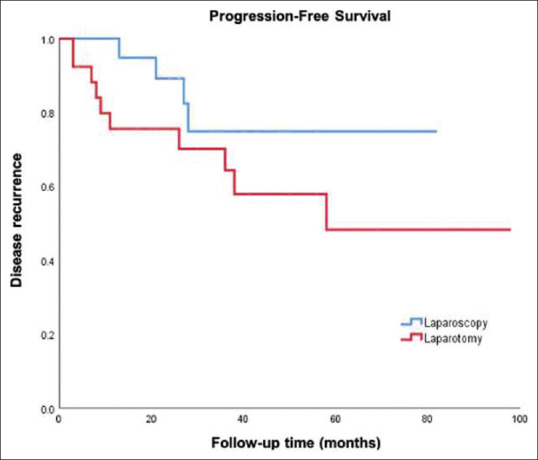
Results: Forty-nine patients were included; of which 20 underwent laparoscopy, 26 laparotomy, and three conversion from laparoscopy to laparotomy. No significant differences were observed between the two groups regarding operative time, number of lymph nodes dissected, or intraoperative tumor rupture rate, while estimated blood loss and transfusion requirements were lower in the laparoscopy group. The complication rate tended to be higher in the laparotomy group. Patients in the laparoscopy group had a faster recovery, with earlier urinary catheter and abdominal drain removal, shorter hospital stay, and a trend toward earlier tolerance of oral diet and mobilization. At a mean follow-up of 45.7 months, 14 patients had disease recurrence, with no differences in the mean progression-free survival between the two groups (36 months for laparoscopy vs. 35.5 months for laparotomy, P = 0.22).
Conclusion: Laparoscopic surgery performed by a trained gynecological oncologist is a safe and effective surgical approach for comprehensive staging of EOC, with the additional benefits of a faster recovery compared to laparotomy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
