Lili Zhang, Yang Hu, Hong Liu, Xue Qi, Hong Chen, Wei Cao, Longsheng Wang, Ye Zhang, Yun Wu
{"title":"Analgesic Efficacy of Combined Thoracic Paravertebral Block and Erector Spinae Plane Block for Video-Assisted Thoracic Surgery: A Prospective Randomized Clinical Trial.","authors":"Lili Zhang, Yang Hu, Hong Liu, Xue Qi, Hong Chen, Wei Cao, Longsheng Wang, Ye Zhang, Yun Wu","doi":"10.12659/MSM.940247","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Thoracic paravertebral block (TPVB) and erector spinae plane block (ESPB) are widely used in video-assisted thoracic surgery (VATS). However, they have corresponding adverse effects, including hypotension for TPVB and unpredictable injectate spread in ESPB. An optimal perioperative analgesic strategy remains controversial. We investigated the effect of ultrasound-guided combined TPVB and ESPB (CTEB) for VATS. MATERIAL AND METHODS A total of 120 patients scheduled for thoracic surgery were randomized to receive either ultrasound-guided TPVB, ESPB, or CTEB preoperatively. Postoperative analgesia was achieved with sufentanil patient-controlled intravenous analgesia. The primary outcome was the static pain score at 2 h after surgery. RESULTS The static pain score 2 h postoperatively was significantly different among the 3 groups. This difference was statistically significant for Group ESPB vs Group TPVB (P=0.004), but not for Group ESPB vs Group CTEB (P=0.767), or Group TPVB vs Group CTEB (P=0.117). Group TPVB exhibited the highest incidence of hypotension among the 3 groups. More patients experienced a sensory loss in Groups TPVB and CTEB 30 min after the block performance. Patients receiving CTEB exhibited a lower incidence of chronic pain 6 months postoperatively than those in Group ESPB. CONCLUSIONS CTEB does not enhance the analgesic effect of ESPB in patients undergoing VATS; however, it may induce a faster sensory loss after nerve block and reduce the incidence of postoperative chronic pain compared with ESPB. CTEB may also help to reduce the incidence of intraoperative hypotension compared with TPVB.</p>","PeriodicalId":18276,"journal":{"name":"Medical Science Monitor : International Medical Journal of Experimental and Clinical Research","volume":"29 ","pages":"e940247"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e2/6d/medscimonit-29-e940247.PMC10334846.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Science Monitor : International Medical Journal of Experimental and Clinical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/MSM.940247","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
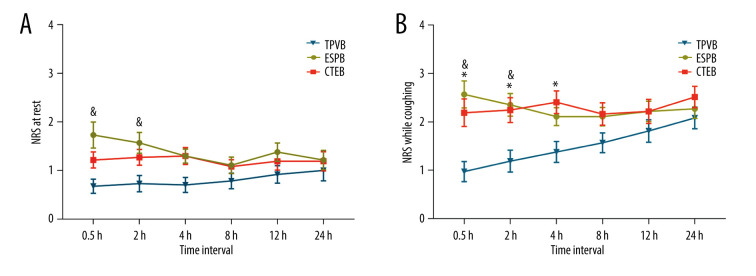
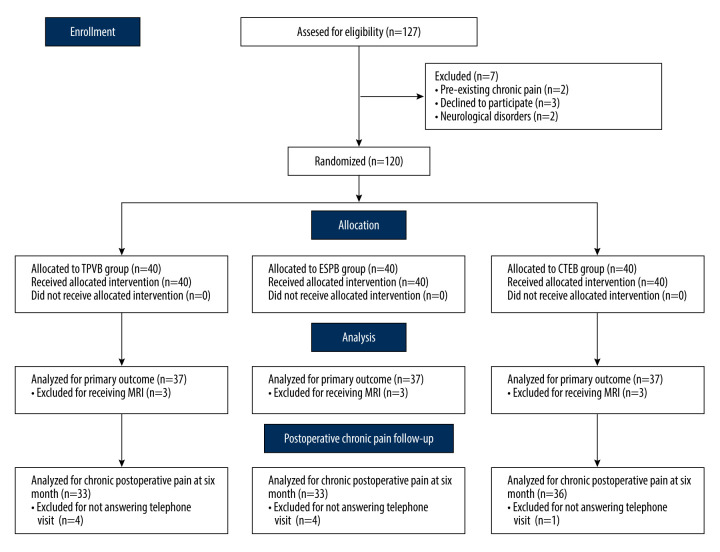
BACKGROUND Thoracic paravertebral block (TPVB) and erector spinae plane block (ESPB) are widely used in video-assisted thoracic surgery (VATS). However, they have corresponding adverse effects, including hypotension for TPVB and unpredictable injectate spread in ESPB. An optimal perioperative analgesic strategy remains controversial. We investigated the effect of ultrasound-guided combined TPVB and ESPB (CTEB) for VATS. MATERIAL AND METHODS A total of 120 patients scheduled for thoracic surgery were randomized to receive either ultrasound-guided TPVB, ESPB, or CTEB preoperatively. Postoperative analgesia was achieved with sufentanil patient-controlled intravenous analgesia. The primary outcome was the static pain score at 2 h after surgery. RESULTS The static pain score 2 h postoperatively was significantly different among the 3 groups. This difference was statistically significant for Group ESPB vs Group TPVB (P=0.004), but not for Group ESPB vs Group CTEB (P=0.767), or Group TPVB vs Group CTEB (P=0.117). Group TPVB exhibited the highest incidence of hypotension among the 3 groups. More patients experienced a sensory loss in Groups TPVB and CTEB 30 min after the block performance. Patients receiving CTEB exhibited a lower incidence of chronic pain 6 months postoperatively than those in Group ESPB. CONCLUSIONS CTEB does not enhance the analgesic effect of ESPB in patients undergoing VATS; however, it may induce a faster sensory loss after nerve block and reduce the incidence of postoperative chronic pain compared with ESPB. CTEB may also help to reduce the incidence of intraoperative hypotension compared with TPVB.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
