Amay Banker, Prashantha Rao, Karthik Ganesan, Ravi Mohanka
{"title":"A fenestrated portal vein.","authors":"Amay Banker, Prashantha Rao, Karthik Ganesan, Ravi Mohanka","doi":"10.4285/kjt.23.0012","DOIUrl":null,"url":null,"abstract":"www.ekjt.org To the Editor: It was a pleasure to read the article by Balradja et al. [1], titled “Portal vein fenestration: a case report of an unusual portal vein developmental anomaly,” published in your journal. The authors have described a rare anatomic variation of the portal vein (PV) and have rightly pointed out the potentially catastrophic consequences of failure to identify such a variation. We report a similar variant and believe that this anatomical configuration deserves further discussion. After appropriate informed consent, we report a similar case of PV fenestration and believe that the anatomical configuration deserves further discussion. We present the case of a 35-year-old woman who was a medically suitable live donor for her husband’s liver transplant. Triphasic computed tomography (CT) showed Nakamura type C PV on maximum intensity projections (MIP). High-resolution (0.6–1.0 mm) reconstruction revealed PV fenestration (Figs. 1A, B, and 2A). The hepatic arterial and venous anatomy were standard and magnetic resonance cholangiography revealed a Huang type IIIB biliary anatomy. During surgery, the right anterior PV (RAPV) and posterior PV (RPPV) were looped separately (Fig. 1C). A trial clamp on the proximal RAPV (Fig. 2B) yielded an ischemic plane between the right anterior and posterior sectors, confirming ongoing portal flow into the anterior sector. Therefore, we clamped the main PV in addition to the right hepatic artery to identify the ischemic line. Subsequent trial clamping of RAPV distal to the fenestration along with RPRV yielded the correct transection plane (Fig. 2C). The RAPV and RPPV were divided separately during graft retrieval (Fig. 1D). Both the donor and recipient had an uneventful recovery. The PV system is formed by the development of the paired vitelline veins and three bridging anastomoses between them. Hemodynamic principles favoring the shortest path following duodenal rotation lead to regression of the caudal ventral anastomosis and the proximal part of the right vitelline vein. The proximal left vitelline vein, the dorsal anastomoses, and the distal right vitelline vein form the main PV. The cranial ventral anastomosis forms the left portal vein. Any deviations from this complex embryonic process lead to the development of PV anomalies such as PV fenestrations [2-4]. We believe that such an anatomy can be erroneously reported as a type C PV on preoperative imaging. Even A fenestrated portal vein","PeriodicalId":33357,"journal":{"name":"Korean Journal of Transplantation","volume":"37 2","pages":"141-143"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/13/59/kjt-37-2-141.PMC10332276.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4285/kjt.23.0012","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
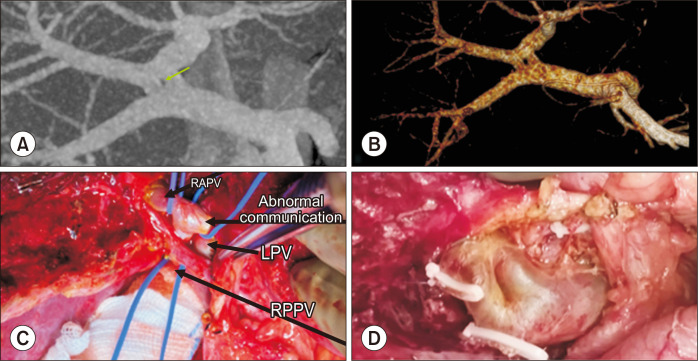
www.ekjt.org To the Editor: It was a pleasure to read the article by Balradja et al. [1], titled “Portal vein fenestration: a case report of an unusual portal vein developmental anomaly,” published in your journal. The authors have described a rare anatomic variation of the portal vein (PV) and have rightly pointed out the potentially catastrophic consequences of failure to identify such a variation. We report a similar variant and believe that this anatomical configuration deserves further discussion. After appropriate informed consent, we report a similar case of PV fenestration and believe that the anatomical configuration deserves further discussion. We present the case of a 35-year-old woman who was a medically suitable live donor for her husband’s liver transplant. Triphasic computed tomography (CT) showed Nakamura type C PV on maximum intensity projections (MIP). High-resolution (0.6–1.0 mm) reconstruction revealed PV fenestration (Figs. 1A, B, and 2A). The hepatic arterial and venous anatomy were standard and magnetic resonance cholangiography revealed a Huang type IIIB biliary anatomy. During surgery, the right anterior PV (RAPV) and posterior PV (RPPV) were looped separately (Fig. 1C). A trial clamp on the proximal RAPV (Fig. 2B) yielded an ischemic plane between the right anterior and posterior sectors, confirming ongoing portal flow into the anterior sector. Therefore, we clamped the main PV in addition to the right hepatic artery to identify the ischemic line. Subsequent trial clamping of RAPV distal to the fenestration along with RPRV yielded the correct transection plane (Fig. 2C). The RAPV and RPPV were divided separately during graft retrieval (Fig. 1D). Both the donor and recipient had an uneventful recovery. The PV system is formed by the development of the paired vitelline veins and three bridging anastomoses between them. Hemodynamic principles favoring the shortest path following duodenal rotation lead to regression of the caudal ventral anastomosis and the proximal part of the right vitelline vein. The proximal left vitelline vein, the dorsal anastomoses, and the distal right vitelline vein form the main PV. The cranial ventral anastomosis forms the left portal vein. Any deviations from this complex embryonic process lead to the development of PV anomalies such as PV fenestrations [2-4]. We believe that such an anatomy can be erroneously reported as a type C PV on preoperative imaging. Even A fenestrated portal vein




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
