{"title":"Clinical and Radiographic Predictors of Successful Coronary Angiography Through Right Radial Artery Access.","authors":"Sohil Elfar, Ahmed Onsy, Mohamed Amr Farouk","doi":"10.15420/icr.2023.04","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: One of the limitations of the right radial access approach is complex vessel anatomy, such as subclavian tortuosity. Several clinical predictors have been proposed for tortuosities, such as older age, female sex and hypertension. In this study, we hypothesised that chest radiography would add predictive value to the traditional predictors. <b>Methods</b>: This prospective blinded study included patients who underwent transradial access coronary angiography. They were classified into four groups according to difficulty: Group I, Group II, Group III and Group IV. Different groups were compared according to clinical and radiographic characteristics. <b>Results</b>: The study included 108 patients (54, 27, 17 and 10 patients in Groups I, II, III and IV, respectively). The rate of crossover to transfemoral access was 9.26%. Age, hypertension and female sex were associated with a greater difficulty and failure rates. Regarding radiographic parameters, a higher failure rate was associated with a higher diameter of the aortic knuckle (Group IV, 4.09 ± 1.32 cm versus Groups I, II and III combined, 3.26 ± 0.98 cm; p=0.015) and the width of the mediastinum (Group IV, 8.96 ± 2.88 cm versus Groups I, II and III combined, 7.28 ± 1.78 cm; p=0.009). The cut-off value for prominent aortic knuckle was 3.55 cm (sensitivity 70% and specificity 67.35%) and the width of mediastinum was 6.59 cm (sensitivity 90% and specificity 42.86%). <b>Conclusion</b>: Radiographic prominent aortic knuckle and wide mediastinum are valuable clinical parameters and useful predictors for transradial access failure caused by tortuosity of the right subclavian/brachiocephalic arteries or aorta.</p>","PeriodicalId":38586,"journal":{"name":"Interventional Cardiology Review","volume":"18 ","pages":"e21"},"PeriodicalIF":2.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9d/6c/icr-18-e21.PMC10331560.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interventional Cardiology Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/icr.2023.04","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"PHILOSOPHY","Score":null,"Total":0}
引用次数: 0
Abstract
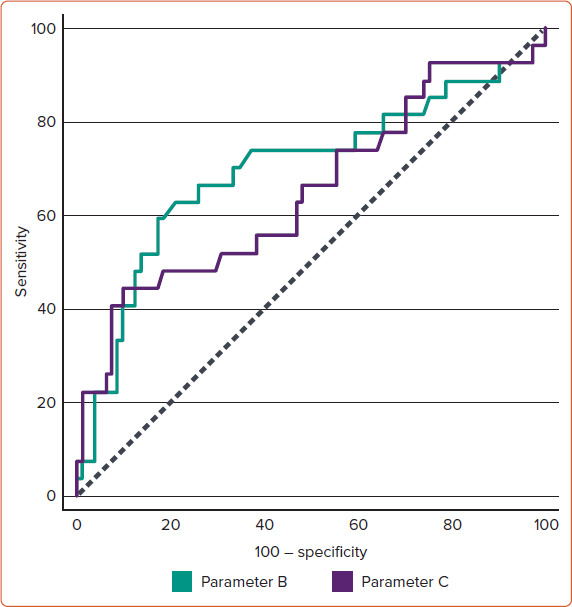
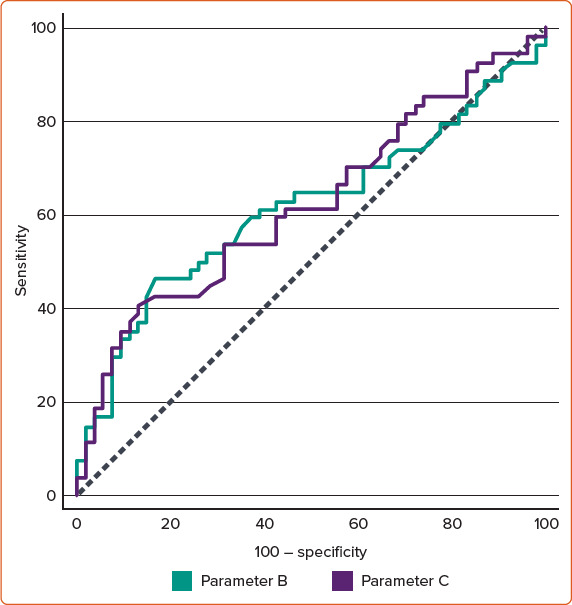
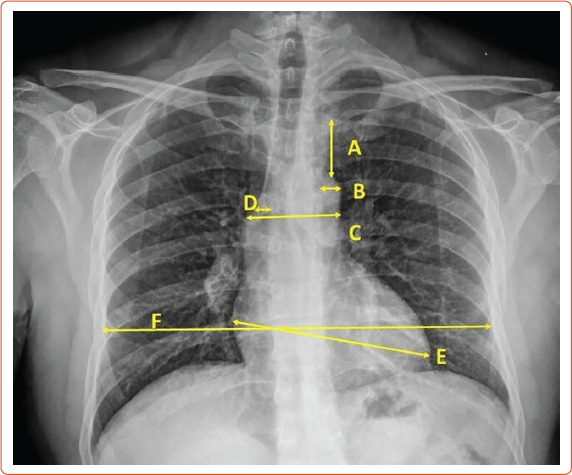
Background: One of the limitations of the right radial access approach is complex vessel anatomy, such as subclavian tortuosity. Several clinical predictors have been proposed for tortuosities, such as older age, female sex and hypertension. In this study, we hypothesised that chest radiography would add predictive value to the traditional predictors. Methods: This prospective blinded study included patients who underwent transradial access coronary angiography. They were classified into four groups according to difficulty: Group I, Group II, Group III and Group IV. Different groups were compared according to clinical and radiographic characteristics. Results: The study included 108 patients (54, 27, 17 and 10 patients in Groups I, II, III and IV, respectively). The rate of crossover to transfemoral access was 9.26%. Age, hypertension and female sex were associated with a greater difficulty and failure rates. Regarding radiographic parameters, a higher failure rate was associated with a higher diameter of the aortic knuckle (Group IV, 4.09 ± 1.32 cm versus Groups I, II and III combined, 3.26 ± 0.98 cm; p=0.015) and the width of the mediastinum (Group IV, 8.96 ± 2.88 cm versus Groups I, II and III combined, 7.28 ± 1.78 cm; p=0.009). The cut-off value for prominent aortic knuckle was 3.55 cm (sensitivity 70% and specificity 67.35%) and the width of mediastinum was 6.59 cm (sensitivity 90% and specificity 42.86%). Conclusion: Radiographic prominent aortic knuckle and wide mediastinum are valuable clinical parameters and useful predictors for transradial access failure caused by tortuosity of the right subclavian/brachiocephalic arteries or aorta.
背景:右桡骨入路的局限性之一是复杂的血管解剖,如锁骨下弯曲。已经提出了一些临床预测因素,如老年、女性和高血压。在这项研究中,我们假设胸部x线摄影可以增加传统预测指标的预测价值。方法:这项前瞻性盲法研究纳入了接受经桡动脉通道冠状动脉造影的患者。根据难易程度分为ⅰ组、ⅱ组、ⅲ组、ⅳ组,并根据临床及影像学特征进行比较。结果:纳入108例患者(I、II、III、IV组分别为54例、27例、17例、10例)。经股交叉通路率为9.26%。年龄、高血压和女性与更大的困难和失败率相关。关于x线参数,更高的失败率与更高的主动脉节直径相关(IV组,4.09±1.32 cm vs . I, II和III组联合,3.26±0.98 cm;p=0.015)和纵隔宽度(IV组为8.96±2.88 cm, I、II、III组合并为7.28±1.78 cm;p = 0.009)。主动脉节突出的截断值为3.55 cm(敏感性70%,特异性67.35%),纵隔宽度为6.59 cm(敏感性90%,特异性42.86%)。结论:主动脉关节突出和纵隔宽是诊断右侧锁骨下/头臂动脉或主动脉扭曲所致桡动脉通路失败的重要临床参数和预测指标。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
