{"title":"How acute myeloid leukemia (AML) escapes from FMS-related tyrosine kinase 3 (FLT3) inhibitors? Still an overrated complication?","authors":"Salvatore Perrone, Tiziana Ottone, Nadezda Zhdanovskaya, Matteo Molica","doi":"10.20517/cdr.2022.130","DOIUrl":null,"url":null,"abstract":"<p><p>FMS-related tyrosine kinase 3 (FLT3) mutations, present in about 25%-30% of acute myeloid leukemia (AML) patients, constitute one of the most frequently detected mutations in these patients. The binding of FLT3L to FLT3 activates the phosphatidylinositol 3-kinase (PI3K) and RAS pathways, producing increased cell proliferation and the inhibition of apoptosis. Two types of FLT3 mutations exist: FLT3-ITD and FLT3-TKD (point mutations in D835 and I836 or deletion of codon I836). A class of drugs, tyrosine-kinase inhibitors (TKI), targeting mutated FLT3, is already available with 1<sup>st</sup> and 2<sup>nd</sup> generation molecules, but only midostaurin and gilteritinib are currently approved. However, the emergence of resistance or the selection of clones not responding to FLT3 inhibitors has become an important clinical dilemma, as the duration of clinical responses is generally limited to a few months. This review analyzes the insights into mechanisms of resistance to TKI and poses a particular view on the clinical relevance of this phenomenon. Has resistance been overlooked? Indeed, FLT3 inhibitors have significantly contributed to reducing the negative impact of FLT3 mutations on the prognosis of AML patients who are no longer considered at high risk by the European LeukemiaNet (ELN) 2022. Finally, several ongoing efforts to overcome resistance to FLT3-inhibitors will be presented: new generation FLT3 inhibitors in monotherapy or combined with standard chemotherapy, hypomethylating drugs, or IDH1/2 inhibitors, Bcl2 inhibitors; novel anti-human FLT3 monoclonal antibodies (e.g., FLT3/CD3 bispecific antibodies); FLT3-CAR T-cells; CDK4/6 kinase inhibitor (e.g., palbociclib).</p>","PeriodicalId":70759,"journal":{"name":"癌症耐药(英文)","volume":"6 2","pages":"223-238"},"PeriodicalIF":4.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10344728/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"癌症耐药(英文)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20517/cdr.2022.130","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
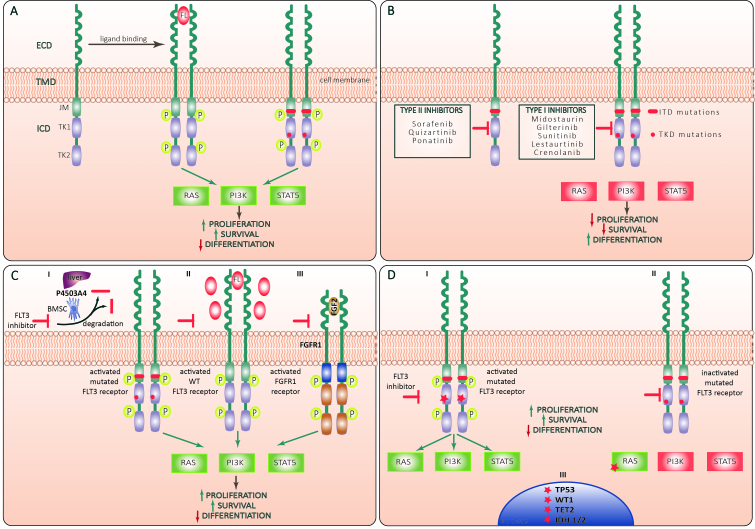
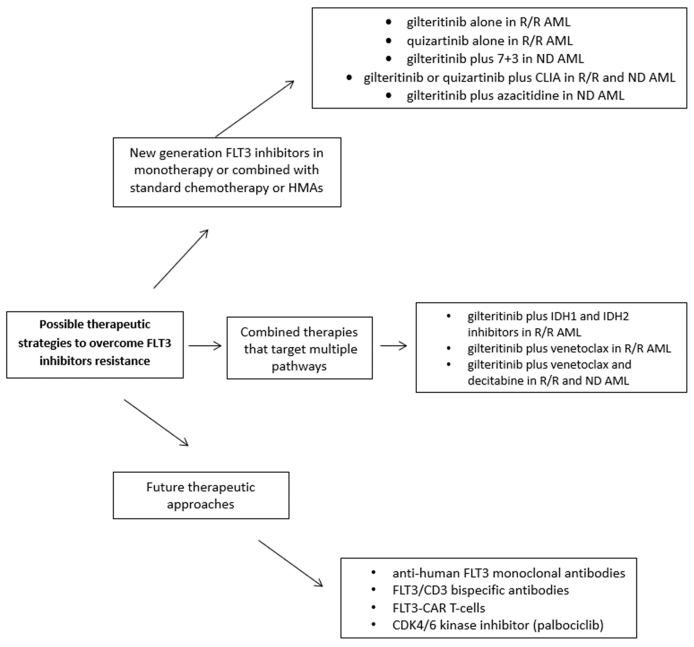
FMS-related tyrosine kinase 3 (FLT3) mutations, present in about 25%-30% of acute myeloid leukemia (AML) patients, constitute one of the most frequently detected mutations in these patients. The binding of FLT3L to FLT3 activates the phosphatidylinositol 3-kinase (PI3K) and RAS pathways, producing increased cell proliferation and the inhibition of apoptosis. Two types of FLT3 mutations exist: FLT3-ITD and FLT3-TKD (point mutations in D835 and I836 or deletion of codon I836). A class of drugs, tyrosine-kinase inhibitors (TKI), targeting mutated FLT3, is already available with 1st and 2nd generation molecules, but only midostaurin and gilteritinib are currently approved. However, the emergence of resistance or the selection of clones not responding to FLT3 inhibitors has become an important clinical dilemma, as the duration of clinical responses is generally limited to a few months. This review analyzes the insights into mechanisms of resistance to TKI and poses a particular view on the clinical relevance of this phenomenon. Has resistance been overlooked? Indeed, FLT3 inhibitors have significantly contributed to reducing the negative impact of FLT3 mutations on the prognosis of AML patients who are no longer considered at high risk by the European LeukemiaNet (ELN) 2022. Finally, several ongoing efforts to overcome resistance to FLT3-inhibitors will be presented: new generation FLT3 inhibitors in monotherapy or combined with standard chemotherapy, hypomethylating drugs, or IDH1/2 inhibitors, Bcl2 inhibitors; novel anti-human FLT3 monoclonal antibodies (e.g., FLT3/CD3 bispecific antibodies); FLT3-CAR T-cells; CDK4/6 kinase inhibitor (e.g., palbociclib).


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
