{"title":"Recurrent laryngeal nerve's course running anteriorly to a thyroid tumor.","authors":"Minoru Kihara, Akira Miyauchi, Makoto Fujishima, Tomo Ishizaka, Akihide Matsunaga, Shiori Kawano, Masashi Yamamoto, Takahiro Sasaki, Hiroo Masuoka, Takuya Higashiyama, Yasuhiro Ito, Naoyoshi Onoda, Akihiro Miya, Takashi Akamizu","doi":"10.1186/s13044-023-00172-6","DOIUrl":null,"url":null,"abstract":"<p><p>The thyroid gland's neurovascular relationship is commonly portrayed as the recurrent laryngeal nerve (RLN) coursing posteriorly to the thyroid gland. We report a rare case with the RLN running anteriorly to a thyroid tumor. A 56-year-old Japanese woman underwent a thyroidectomy for a benign thyroid tumor. Preoperatively, computed tomography confirmed that part of the tumor had extended into the mediastinum and was descending posteriorly up to the brachiocephalic artery. Intraoperatively, when the sternothyroid muscle was incised to expose the thyroid gland, a cord (nerve)-like structure was observed directly anterior to the thyroid tumor. Although the course of this cord-like structure was clearly different from the \"traditional\" course of the right RLN, the possibility that the structure was the RLN could not be excluded. The structure was traced back in order to preserve it; we saw that it entered the larynx at the lower margin of the cricothyroid muscle and approximately at the level of the cricothyroid junction through the back of the normal thyroid tissue. With intraoperative neuromonitoring, the structure was identified as the RLN. As a result, the course of the RLN run anterior to the tumor but then posterior to the 'normal thyroid' i.e. into it normal anatomical position. Had we assumed that the RLN was behind the thyroid tumor, we would have damaged the RLN. It would not be possible to diagnose this abnormal running course of the RLN reliably before surgery, but extra care should be taken in similar cases, that is, when a large thyroid tumor is descending posteriorly up to the brachiocephalic artery on the right side.</p>","PeriodicalId":39048,"journal":{"name":"Thyroid Research","volume":"16 1","pages":"30"},"PeriodicalIF":1.8000,"publicationDate":"2023-07-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10357722/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-023-00172-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
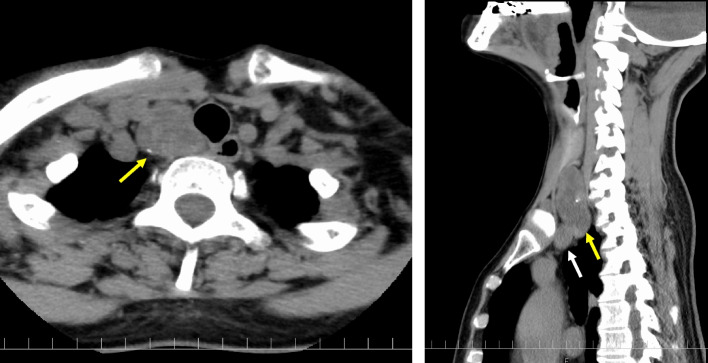
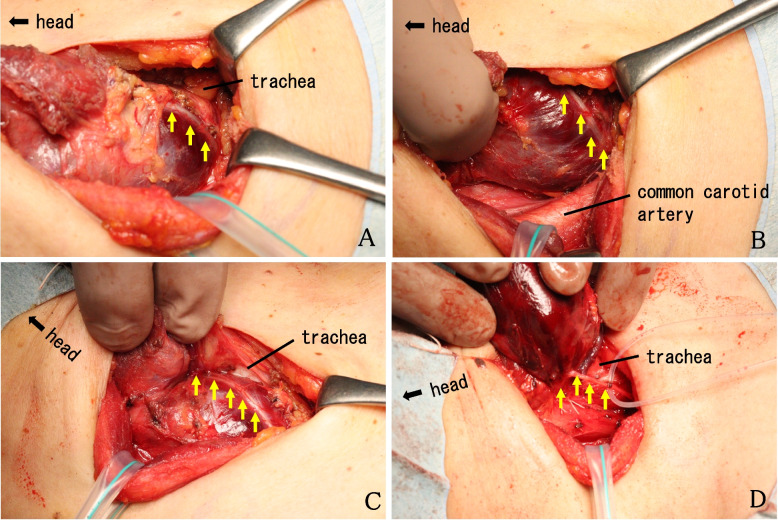
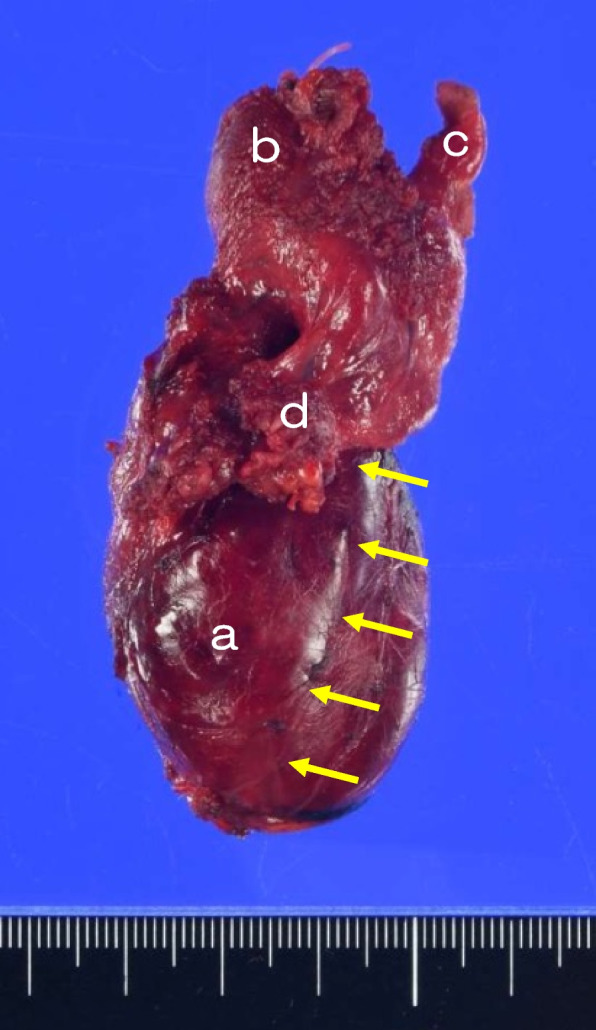
The thyroid gland's neurovascular relationship is commonly portrayed as the recurrent laryngeal nerve (RLN) coursing posteriorly to the thyroid gland. We report a rare case with the RLN running anteriorly to a thyroid tumor. A 56-year-old Japanese woman underwent a thyroidectomy for a benign thyroid tumor. Preoperatively, computed tomography confirmed that part of the tumor had extended into the mediastinum and was descending posteriorly up to the brachiocephalic artery. Intraoperatively, when the sternothyroid muscle was incised to expose the thyroid gland, a cord (nerve)-like structure was observed directly anterior to the thyroid tumor. Although the course of this cord-like structure was clearly different from the "traditional" course of the right RLN, the possibility that the structure was the RLN could not be excluded. The structure was traced back in order to preserve it; we saw that it entered the larynx at the lower margin of the cricothyroid muscle and approximately at the level of the cricothyroid junction through the back of the normal thyroid tissue. With intraoperative neuromonitoring, the structure was identified as the RLN. As a result, the course of the RLN run anterior to the tumor but then posterior to the 'normal thyroid' i.e. into it normal anatomical position. Had we assumed that the RLN was behind the thyroid tumor, we would have damaged the RLN. It would not be possible to diagnose this abnormal running course of the RLN reliably before surgery, but extra care should be taken in similar cases, that is, when a large thyroid tumor is descending posteriorly up to the brachiocephalic artery on the right side.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
