Successful Sirolimus Treatment for Recurrent Pericardial Effusion in a Large Cervicomediastinal Provisionally Unclassified Vascular Anomaly: A Case Report.
Julio César Moreno-Alfonso, María San Basilio Berenguer, María Del Carmen Sarmiento Caldas, Jesús González Cayón, Santiago de la Puente, Paloma Triana, Juan Carlos López-Gutiérrez
{"title":"Successful Sirolimus Treatment for Recurrent Pericardial Effusion in a Large Cervicomediastinal Provisionally Unclassified Vascular Anomaly: A Case Report.","authors":"Julio César Moreno-Alfonso, María San Basilio Berenguer, María Del Carmen Sarmiento Caldas, Jesús González Cayón, Santiago de la Puente, Paloma Triana, Juan Carlos López-Gutiérrez","doi":"10.1055/a-2057-7177","DOIUrl":null,"url":null,"abstract":"<p><p>Provisionally unclassified vascular anomalies (PUVA) are a group of diseases with unique characteristics that make them unclassifiable within vascular tumors or malformations. We describe a PUVA as the cause of recurrent pericardial effusion and its response to sirolimus. A 6-year-old girl was referred with a cervicothoracic vascular anomaly, a violaceous, and irregular lesion in the neck and upper chest, diagnosed as \"hemangioma\". She had pericardial effusion at the neonatal age that required pericardiocentesis, propranolol, and corticosteroids. She remained stable for 5 years, when she presented with a severe pericardial effusion. A magnetic resonance visualized a diffuse vascular image in the cervical and thoracic region with mediastinal extension. The pathological study showed a vascular proliferation in the dermis and hypodermis with positive staining for Wilms' Tumor 1 Protein (WT1) and negative for Glut-1. Genetic testing found a variant in <i>GNA14</i> , for which the diagnosis of PUVA was established. When a pericardial drain was placed without response, treatment with sirolimus was started with resolution of the effusion. Sixteen months later, the malformation is stable and there has been no recurrence of pericardial effusion. In a significant group of patients, definitive diagnosis is not possible despite pathological and genetic analysis. Mammalian target of rapamycin inhibitors may become a therapeutic option if symptoms are severe enough, with a low rate of reported side effects.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":"11 1","pages":"e20-e24"},"PeriodicalIF":0.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10191730/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2057-7177","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
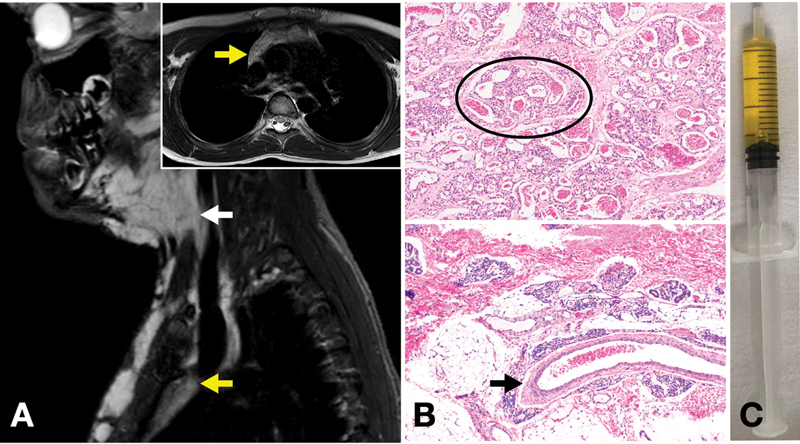
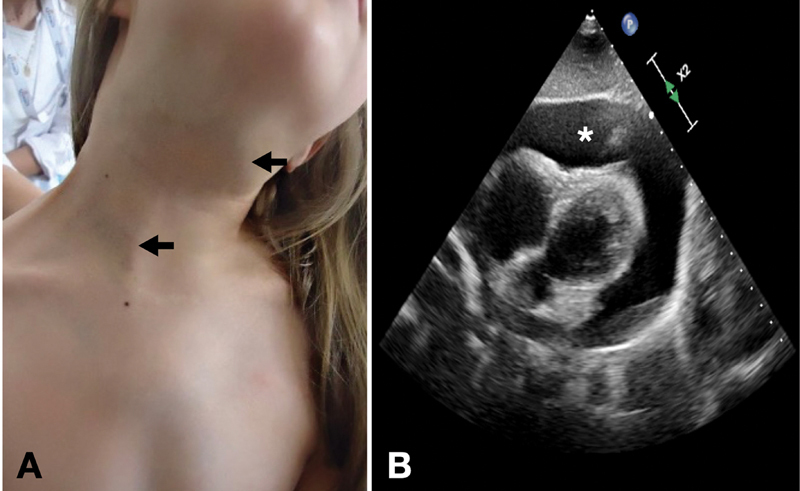
Provisionally unclassified vascular anomalies (PUVA) are a group of diseases with unique characteristics that make them unclassifiable within vascular tumors or malformations. We describe a PUVA as the cause of recurrent pericardial effusion and its response to sirolimus. A 6-year-old girl was referred with a cervicothoracic vascular anomaly, a violaceous, and irregular lesion in the neck and upper chest, diagnosed as "hemangioma". She had pericardial effusion at the neonatal age that required pericardiocentesis, propranolol, and corticosteroids. She remained stable for 5 years, when she presented with a severe pericardial effusion. A magnetic resonance visualized a diffuse vascular image in the cervical and thoracic region with mediastinal extension. The pathological study showed a vascular proliferation in the dermis and hypodermis with positive staining for Wilms' Tumor 1 Protein (WT1) and negative for Glut-1. Genetic testing found a variant in GNA14 , for which the diagnosis of PUVA was established. When a pericardial drain was placed without response, treatment with sirolimus was started with resolution of the effusion. Sixteen months later, the malformation is stable and there has been no recurrence of pericardial effusion. In a significant group of patients, definitive diagnosis is not possible despite pathological and genetic analysis. Mammalian target of rapamycin inhibitors may become a therapeutic option if symptoms are severe enough, with a low rate of reported side effects.
暂未分类血管异常(PUVA)是一组具有独特特征的疾病,使其在血管肿瘤或畸形中无法分类。我们将PUVA描述为复发性心包积液的原因及其对西罗莫司的反应。一个6岁的女孩被转诊颈胸血管异常,颈部和上胸部的紫色和不规则病变,诊断为“血管瘤”。她在新生儿时有心包积液,需要心包穿刺、心得安和皮质类固醇。在出现严重的心包积液时,患者病情稳定了5年。磁共振显示颈、胸区域弥漫性血管图像,纵隔延伸。病理观察显示真皮和下皮层血管增生,Wilms' Tumor 1 Protein (WT1)阳性,Glut-1阴性。基因检测发现了GNA14的变异,从而确定了PUVA的诊断。当心包引流无反应时,随着积液的溶解开始使用西罗莫司治疗。16个月后,畸形稳定,没有再出现心包积液。在一组显著的患者,明确的诊断是不可能的,尽管病理和遗传分析。哺乳动物靶向雷帕霉素抑制剂可能成为一种治疗选择,如果症状足够严重,报告的副作用率低。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
