Rationale and design of Tenecteplase Reperfusion Therapy in Acute Ischaemic Cerebrovascular Events III (TRACE III): a randomised, phase III, open-label, controlled trial.
Yunyun Xiong, Bruce C V Campbell, Marc Fisher, Lee H Schwamm, Mark Parsons, Hao Li, Yuesong Pan, Xia Meng, Xingquan Zhao, Yongjun Wang
{"title":"Rationale and design of Tenecteplase Reperfusion Therapy in Acute Ischaemic Cerebrovascular Events III (TRACE III): a randomised, phase III, open-label, controlled trial.","authors":"Yunyun Xiong, Bruce C V Campbell, Marc Fisher, Lee H Schwamm, Mark Parsons, Hao Li, Yuesong Pan, Xia Meng, Xingquan Zhao, Yongjun Wang","doi":"10.1136/svn-2023-002310","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Recombinant human TNK tissue-type plasminogen activator (rhTNK-tPA) was not inferior to alteplase for ischaemic stroke within 4.5 hours. Our study aimed to investigate the efficacy and safety of rhTNK-tPA in patients who had an ischaemic stroke due to large vessel occlusion (LVO) of anterior circulation beyond 4.5 hours.</p><p><strong>Methods and design: </strong>Tenecteplase Reperfusion Therapy in Acute Ischaemic Cerebrovascular Events-III (TRACE III) is a multicentre, prospective, randomised, open-label, blind endpoint, controlled clinical trial. Patients who had an ischaemic stroke due to anterior circulation LVO (internal carotid artery, middle cerebral artery M1 and M2 segments) within 4.5-24 hours from last known well (including wake-up stroke and no witness stroke) and with salvageable tissue (ischaemic core volume <70 mL, mismatch ratio ≥1.8 and mismatch volume ≥15 mL) based on CT perfusion or MRI perfusion-weighted imaging (PWI) were included and randomised to rhTNK-tPA 0.25 mg/kg (single bolus) to a maximum of 25 mg or standard medical therapy. Specially, we will exclude patients who are intended for direct thrombectomy. All will be followed up for 90 days.</p><p><strong>Study outcomes: </strong>Primary efficacy outcome is modified Rankin Scale (mRS) score ≤1 at 90 days. Secondary efficacy outcomes include ordinal distribution of mRS at 90 days, major neurological improvement defined by a decrease ≥8 points compared with the initial deficit or a score ≤1 on the National Institutes of Health Stroke Scale (NIHSS) at 72 hours, mRS score ≤2 at 90 days, the rate of improvement on Tmax >6 s at 24 hours and NIHSS score change from baseline at 7 days. Safety outcomes are symptomatic intracerebral haemorrhage within 36 hours and mortality at 90 days.</p><p><strong>Discussion: </strong>TRACE III will provide evidence for the efficacy and safety of rhTNK-tPA in patients who had an ischaemic strokes due to anterior circulation LVO beyond 4.5 hours.</p><p><strong>Trial registration number: </strong>NCT05141305.</p>","PeriodicalId":22021,"journal":{"name":"Stroke and Vascular Neurology","volume":" ","pages":"82-89"},"PeriodicalIF":4.9000,"publicationDate":"2024-02-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10956103/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke and Vascular Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2023-002310","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: Recombinant human TNK tissue-type plasminogen activator (rhTNK-tPA) was not inferior to alteplase for ischaemic stroke within 4.5 hours. Our study aimed to investigate the efficacy and safety of rhTNK-tPA in patients who had an ischaemic stroke due to large vessel occlusion (LVO) of anterior circulation beyond 4.5 hours.
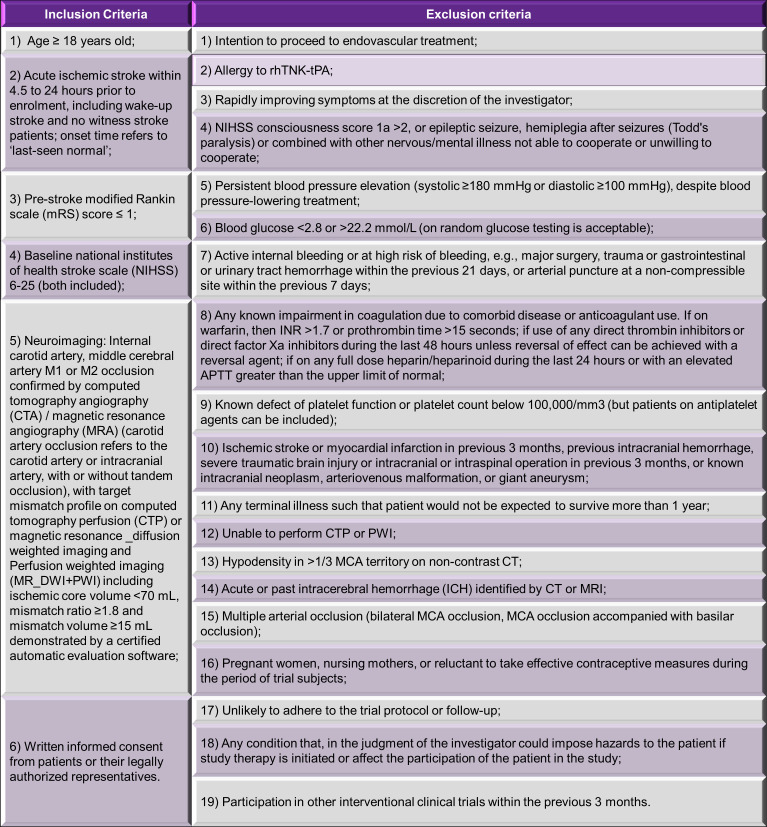
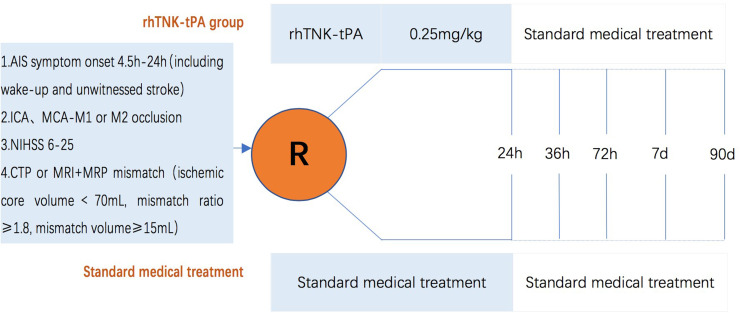
Methods and design: Tenecteplase Reperfusion Therapy in Acute Ischaemic Cerebrovascular Events-III (TRACE III) is a multicentre, prospective, randomised, open-label, blind endpoint, controlled clinical trial. Patients who had an ischaemic stroke due to anterior circulation LVO (internal carotid artery, middle cerebral artery M1 and M2 segments) within 4.5-24 hours from last known well (including wake-up stroke and no witness stroke) and with salvageable tissue (ischaemic core volume <70 mL, mismatch ratio ≥1.8 and mismatch volume ≥15 mL) based on CT perfusion or MRI perfusion-weighted imaging (PWI) were included and randomised to rhTNK-tPA 0.25 mg/kg (single bolus) to a maximum of 25 mg or standard medical therapy. Specially, we will exclude patients who are intended for direct thrombectomy. All will be followed up for 90 days.
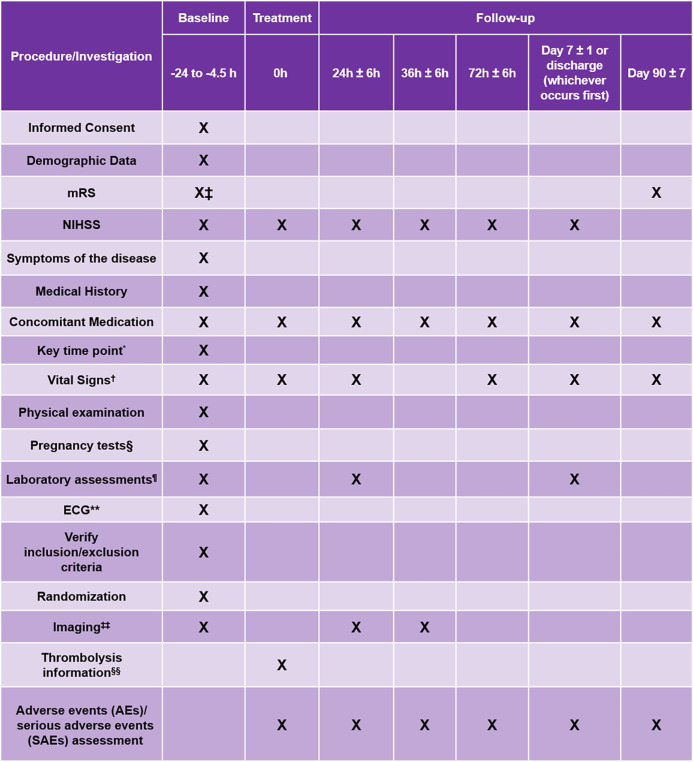
Study outcomes: Primary efficacy outcome is modified Rankin Scale (mRS) score ≤1 at 90 days. Secondary efficacy outcomes include ordinal distribution of mRS at 90 days, major neurological improvement defined by a decrease ≥8 points compared with the initial deficit or a score ≤1 on the National Institutes of Health Stroke Scale (NIHSS) at 72 hours, mRS score ≤2 at 90 days, the rate of improvement on Tmax >6 s at 24 hours and NIHSS score change from baseline at 7 days. Safety outcomes are symptomatic intracerebral haemorrhage within 36 hours and mortality at 90 days.
Discussion: TRACE III will provide evidence for the efficacy and safety of rhTNK-tPA in patients who had an ischaemic strokes due to anterior circulation LVO beyond 4.5 hours.
期刊介绍:
Stroke and Vascular Neurology (SVN) is the official journal of the Chinese Stroke Association. Supported by a team of renowned Editors, and fully Open Access, the journal encourages debate on controversial techniques, issues on health policy and social medicine.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
