Marek Hozman, Sabri Hassouna, Lukas Grochol, Petr Waldauf, Tomas Hracek, Blanka Zborilova Pazdiorova, Stanislav Adamec, Pavel Osmancik
{"title":"Previous antithrombotic therapy does not have an impact on the in-hospital mortality of patients with upper gastrointestinal bleeding.","authors":"Marek Hozman, Sabri Hassouna, Lukas Grochol, Petr Waldauf, Tomas Hracek, Blanka Zborilova Pazdiorova, Stanislav Adamec, Pavel Osmancik","doi":"10.1093/eurheartjsupp/suad103","DOIUrl":null,"url":null,"abstract":"<p><p>The association between antithrombotics (ATs) and the risk of gastrointestinal bleeding is well known; however, data regarding the influence of ATs on outcomes are scarce. The goals of this study are: (i) to assess the impact of prior AT therapy on in-hospital and 6-month outcomes and (ii) to determine the re-initiation rate of the ATs after a bleeding event. All patients with upper gastrointestinal bleeding (UGB) who underwent urgent gastroscopy in three centres from 1 January 2019 to 31 December 2019 were retrospectively analysed. Propensity score matching (PSM) was used. Among 333 patients [60% males, mean age 69.2 (±17.3) years], 44% were receiving ATs. In multivariate logistic regression, no association between AT treatment and worse in-hospital outcomes was observed. Development of haemorrhagic shock led to worse survival [odds ratio (OR) 4.4, 95% confidence interval (CI) 1.9-10.2, <i>P</i> < 0.001; after PSM: OR 5.3, 95% CI 1.8-15.7, <i>P</i> = 0.003]. During 6-months follow-up, higher age (OR 1.0, 95% CI 1.0-1.1, <i>P</i> = 0.002), higher comorbidity (OR 1.4, 95% CI 1.2-1.7, <i>P</i> < 0.001), a history of cancer (OR 3.6, 95% CI 1.6-8.1, <i>P</i> < 0.001) and a history of liver cirrhosis (OR 2.2, 95% CI 1.0-4.4, <i>P</i> = 0.029) were associated with higher mortality. After a bleeding episode, ATs were adequately re-initiated in 73.8%. Previous AT therapy does not worsen in-hospital outcomes in after UGB. Development of haemorrhagic shock predicted poor prognosis. Higher 6-month mortality was observed in older patients, patients with more comorbidities, with liver cirrhosis and cancer.</p>","PeriodicalId":11956,"journal":{"name":"European Heart Journal Supplements","volume":"25 Suppl E","pages":"E25-E32"},"PeriodicalIF":1.7000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/07/80/suad103.PMC10206644.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal Supplements","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/eurheartjsupp/suad103","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
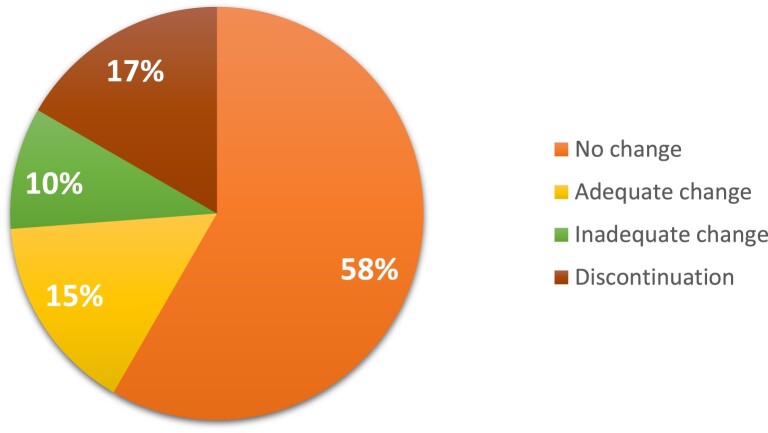
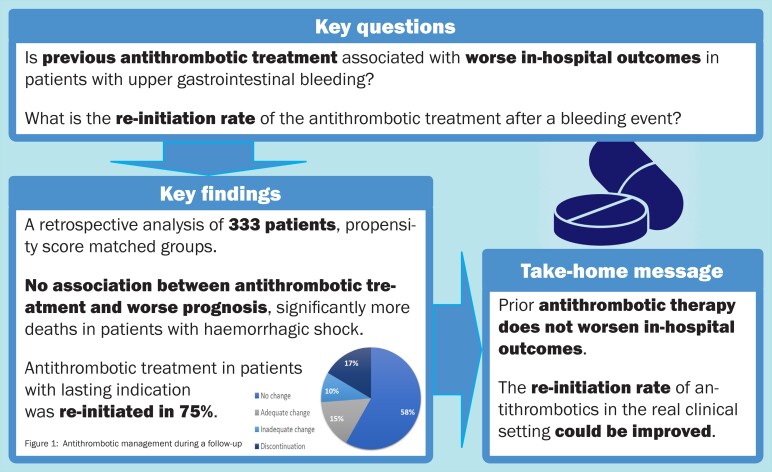
The association between antithrombotics (ATs) and the risk of gastrointestinal bleeding is well known; however, data regarding the influence of ATs on outcomes are scarce. The goals of this study are: (i) to assess the impact of prior AT therapy on in-hospital and 6-month outcomes and (ii) to determine the re-initiation rate of the ATs after a bleeding event. All patients with upper gastrointestinal bleeding (UGB) who underwent urgent gastroscopy in three centres from 1 January 2019 to 31 December 2019 were retrospectively analysed. Propensity score matching (PSM) was used. Among 333 patients [60% males, mean age 69.2 (±17.3) years], 44% were receiving ATs. In multivariate logistic regression, no association between AT treatment and worse in-hospital outcomes was observed. Development of haemorrhagic shock led to worse survival [odds ratio (OR) 4.4, 95% confidence interval (CI) 1.9-10.2, P < 0.001; after PSM: OR 5.3, 95% CI 1.8-15.7, P = 0.003]. During 6-months follow-up, higher age (OR 1.0, 95% CI 1.0-1.1, P = 0.002), higher comorbidity (OR 1.4, 95% CI 1.2-1.7, P < 0.001), a history of cancer (OR 3.6, 95% CI 1.6-8.1, P < 0.001) and a history of liver cirrhosis (OR 2.2, 95% CI 1.0-4.4, P = 0.029) were associated with higher mortality. After a bleeding episode, ATs were adequately re-initiated in 73.8%. Previous AT therapy does not worsen in-hospital outcomes in after UGB. Development of haemorrhagic shock predicted poor prognosis. Higher 6-month mortality was observed in older patients, patients with more comorbidities, with liver cirrhosis and cancer.
抗血栓药物(ATs)与胃肠道出血风险之间的关联是众所周知的;然而,关于ATs对结果影响的数据很少。本研究的目的是:(i)评估先前AT治疗对住院和6个月预后的影响;(ii)确定出血事件后AT的重新启动率。回顾性分析2019年1月1日至2019年12月31日在三个中心接受紧急胃镜检查的所有上消化道出血(UGB)患者。采用倾向评分匹配(PSM)。333例患者中(60%为男性,平均年龄69.2(±17.3)岁),44%接受ATs治疗。在多变量logistic回归中,未观察到AT治疗与较差的住院预后之间的关联。发生出血性休克导致生存率降低[优势比(OR) 4.4, 95%可信区间(CI) 1.9 ~ 10.2, P < 0.001;PSM后:OR 5.3, 95% CI 1.8 ~ 15.7, P = 0.003]。在6个月的随访中,较高的年龄(OR 1.0, 95% CI 1.0-1.1, P = 0.002)、较高的合并症(OR 1.4, 95% CI 1.2-1.7, P < 0.001)、癌症史(OR 3.6, 95% CI 1.6-8.1, P < 0.001)和肝硬化史(OR 2.2, 95% CI 1.0-4.4, P = 0.029)与较高的死亡率相关。出血发作后,73.8%的患者充分重新启动了ATs。先前的AT治疗不会使UGB后的住院结果恶化。出血性休克的发生预示预后不良。老年患者、合并症较多、肝硬化和癌症患者6个月死亡率较高。
期刊介绍:
The European Heart Journal Supplements (EHJs) is a long standing member of the ESC Journal Family that serves as a publication medium for supplemental issues of the flagship European Heart Journal. Traditionally EHJs published a broad range of articles from symposia to special issues on specific topics of interest.
The Editor-in-Chief, Professor Roberto Ferrari, together with his team of eminent Associate Editors: Professor Francisco Fernández-Avilés, Professors Jeroen Bax, Michael Böhm, Frank Ruschitzka, and Thomas Lüscher from the European Heart Journal, has implemented a change of focus for the journal. This entirely refreshed version of the European Heart Journal Supplements now bears the subtitle the Heart of the Matter to give recognition to the focus the journal now has.
The EHJs – the Heart of the Matter intends to offer a dedicated, scientific space for the ESC, Institutions, National and Affiliate Societies, Associations, Working Groups and Councils to disseminate their important successes globally.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
