Rationale and design of a randomised double-blind 2×2 factorial trial comparing the effect of a 3-month intensive statin and antiplatelet therapy for patients with acute mild ischaemic stroke or high-risk TIA with intracranial or extracranial atherosclerosis (INSPIRES).
Ying Gao, Yuesong Pan, Shangrong Han, Weiqi Chen, Jing Jing, Chunjuan Wang, Yingying Yang, Tingting Wang, Xia Meng, Xingquan Zhao, Liping Liu, Hao Li, S Claiborne Johnston, Pierre Amarenco, Philip M Bath, Yongjun Wang, Yilong Wang
{"title":"Rationale and design of a randomised double-blind 2×2 factorial trial comparing the effect of a 3-month intensive statin and antiplatelet therapy for patients with acute mild ischaemic stroke or high-risk TIA with intracranial or extracranial atherosclerosis (INSPIRES).","authors":"Ying Gao, Yuesong Pan, Shangrong Han, Weiqi Chen, Jing Jing, Chunjuan Wang, Yingying Yang, Tingting Wang, Xia Meng, Xingquan Zhao, Liping Liu, Hao Li, S Claiborne Johnston, Pierre Amarenco, Philip M Bath, Yongjun Wang, Yilong Wang","doi":"10.1136/svn-2022-002084","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>It remains unclear if intensive antiplatelet and statin treatments begun within 24-72 hours of cerebral ischaemic events from intracranial or extracranial atherosclerosis is effective or safe.</p><p><strong>Methods: </strong>The Intensive Statin and Antiplatelet Therapy for High-risk Intracranial or Extracranial Atherosclerosis (INSPIRES) trial is a randomised, double-blind, placebo-controlled, multicentre and 2×2 factorial trial. 6100 individuals between the ages of 35 and 80 who have experienced a mild ischaemic stroke or high-risk transient ischaemic attack (TIA) within the previous 72 hours that is attributed to ≥50% atherosclerotic stenosis of a major intracranial or extracranial artery or multiple infarctions of atherosclerotic origin will be enrolled in the trial. Eligible subjects will be randomised 1:1:1:1 to one of four groups: (1) intensive antiplatelet therapy (combined clopidogrel and aspirin for days 1-21, then aspirin placebo and clopidogrel for days 22-90) plus immediate intensive statin therapy(atorvastatin at a dose of 80 mg daily for the first 21 days, then 40 mg daily for days 22-90); (2) intensive antiplatelet therapy plus delayed intensive statin therapy (atorvastatin placebo for days 1-3, followed by 40 mg per day of atorvastatin for days 4-90); (3) standard antiplatelet therapy (combination of clopidogrel placebo with aspirin for 90 days) plus immediate intensive statin therapy and (4) standard antiplatelet therapy plus delayed intensive statin therapy. The primary efficacy endpoint is any new stroke (ischaemic or haemorrhagic) within 90 days after randomisation. The primary safety endpoint is moderate to severe bleeding at 90 days.</p><p><strong>Conclusion: </strong>The INSPIRES trial will assess the efficacy and safety of intensive antiplatelet therapy and immediate intensive statin therapy begun within 72 hours of onset in decreasing the recurrent stroke at 90 days in patients with acute mild ischaemic stroke or high-risk TIA of intracranial or extracranial atherosclerosis origin.</p><p><strong>Trial registration number: </strong>NCT03635749.</p>","PeriodicalId":22021,"journal":{"name":"Stroke and Vascular Neurology","volume":"8 3","pages":"249-258"},"PeriodicalIF":4.9000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c1/0d/svn-2022-002084.PMC10359782.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke and Vascular Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2022-002084","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: It remains unclear if intensive antiplatelet and statin treatments begun within 24-72 hours of cerebral ischaemic events from intracranial or extracranial atherosclerosis is effective or safe.
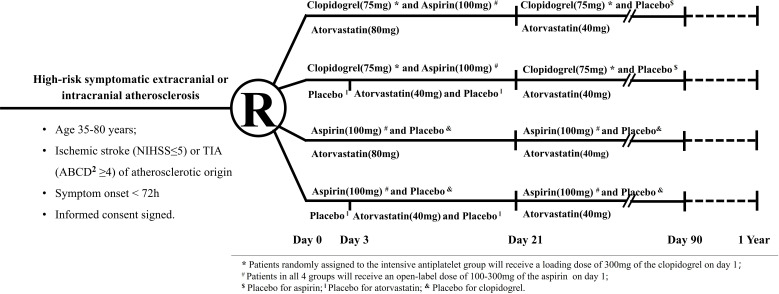
Methods: The Intensive Statin and Antiplatelet Therapy for High-risk Intracranial or Extracranial Atherosclerosis (INSPIRES) trial is a randomised, double-blind, placebo-controlled, multicentre and 2×2 factorial trial. 6100 individuals between the ages of 35 and 80 who have experienced a mild ischaemic stroke or high-risk transient ischaemic attack (TIA) within the previous 72 hours that is attributed to ≥50% atherosclerotic stenosis of a major intracranial or extracranial artery or multiple infarctions of atherosclerotic origin will be enrolled in the trial. Eligible subjects will be randomised 1:1:1:1 to one of four groups: (1) intensive antiplatelet therapy (combined clopidogrel and aspirin for days 1-21, then aspirin placebo and clopidogrel for days 22-90) plus immediate intensive statin therapy(atorvastatin at a dose of 80 mg daily for the first 21 days, then 40 mg daily for days 22-90); (2) intensive antiplatelet therapy plus delayed intensive statin therapy (atorvastatin placebo for days 1-3, followed by 40 mg per day of atorvastatin for days 4-90); (3) standard antiplatelet therapy (combination of clopidogrel placebo with aspirin for 90 days) plus immediate intensive statin therapy and (4) standard antiplatelet therapy plus delayed intensive statin therapy. The primary efficacy endpoint is any new stroke (ischaemic or haemorrhagic) within 90 days after randomisation. The primary safety endpoint is moderate to severe bleeding at 90 days.
Conclusion: The INSPIRES trial will assess the efficacy and safety of intensive antiplatelet therapy and immediate intensive statin therapy begun within 72 hours of onset in decreasing the recurrent stroke at 90 days in patients with acute mild ischaemic stroke or high-risk TIA of intracranial or extracranial atherosclerosis origin.
期刊介绍:
Stroke and Vascular Neurology (SVN) is the official journal of the Chinese Stroke Association. Supported by a team of renowned Editors, and fully Open Access, the journal encourages debate on controversial techniques, issues on health policy and social medicine.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
