Safety of low-dose anticoagulation in extracorporeal membrane oxygenation using the Permanent Life Support System: a retrospective observational study.
{"title":"Safety of low-dose anticoagulation in extracorporeal membrane oxygenation using the Permanent Life Support System: a retrospective observational study.","authors":"Kyungsub Song, Jae Bum Kim","doi":"10.12701/jyms.2023.00339","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bleeding and thrombosis are major complications associated with high mortality in extracorporeal membrane oxygenation (ECMO) management. Anticoagulant therapy should be adequate to reduce thrombosis. However, related studies are limited.</p><p><strong>Methods: </strong>We retrospectively reviewed all patients supported with ECMO at a single institution between January 2014 and July 2022 and included those on all types of ECMO using the Permanent Life Support System. Patients were classified into two groups according to their measured mean activated partial thromboplastin time (aPTT) during ECMO management: a high-anticoagulation (AC) group (aPTT, ≥55 seconds; n=52) and a low-AC group (aPTT, <55 seconds; n=79). The primary outcome was thrombotic or bleeding events during ECMO.</p><p><strong>Results: </strong>We identified 10 patients with bleeding; significantly more of these patients were in the high-AC group (n=8) than in the low-AC group (15.4% vs. 2.5%, p=0.01). However, thrombus events and oxygenator change-free times were not significantly different between the two groups. Four patients in the high-AC group died of bleeding complications (brain hemorrhage, two; hemopericardium, one; and gastrointestinal bleeding, one). One patient in the low-AC group developed a thrombus and died of ECMO dysfunction due to circuit thrombosis.</p><p><strong>Conclusion: </strong>Heparin did not significantly improve thrombotic outcomes. However, maintaining an aPTT of ≥55 seconds was a significant risk factor for bleeding events, especially those associated with mortality.</p>","PeriodicalId":74020,"journal":{"name":"Journal of Yeungnam medical science","volume":"40 3","pages":"276-282"},"PeriodicalIF":1.4000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7e/75/jyms-2023-00339.PMC10390269.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Yeungnam medical science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12701/jyms.2023.00339","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Bleeding and thrombosis are major complications associated with high mortality in extracorporeal membrane oxygenation (ECMO) management. Anticoagulant therapy should be adequate to reduce thrombosis. However, related studies are limited.
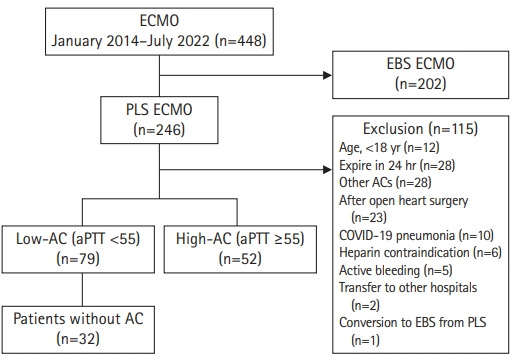
Methods: We retrospectively reviewed all patients supported with ECMO at a single institution between January 2014 and July 2022 and included those on all types of ECMO using the Permanent Life Support System. Patients were classified into two groups according to their measured mean activated partial thromboplastin time (aPTT) during ECMO management: a high-anticoagulation (AC) group (aPTT, ≥55 seconds; n=52) and a low-AC group (aPTT, <55 seconds; n=79). The primary outcome was thrombotic or bleeding events during ECMO.
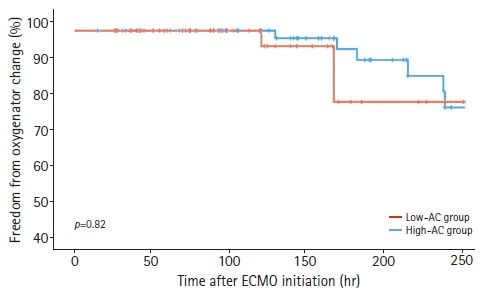
Results: We identified 10 patients with bleeding; significantly more of these patients were in the high-AC group (n=8) than in the low-AC group (15.4% vs. 2.5%, p=0.01). However, thrombus events and oxygenator change-free times were not significantly different between the two groups. Four patients in the high-AC group died of bleeding complications (brain hemorrhage, two; hemopericardium, one; and gastrointestinal bleeding, one). One patient in the low-AC group developed a thrombus and died of ECMO dysfunction due to circuit thrombosis.
Conclusion: Heparin did not significantly improve thrombotic outcomes. However, maintaining an aPTT of ≥55 seconds was a significant risk factor for bleeding events, especially those associated with mortality.
背景:出血和血栓形成是体外膜氧合(ECMO)治疗中死亡率高的主要并发症。抗凝治疗应足以减少血栓形成。然而,相关研究有限。方法:我们回顾性分析了2014年1月至2022年7月在一家机构接受ECMO支持的所有患者,包括使用永久生命支持系统的所有类型ECMO患者。根据ECMO管理期间测量的平均活化部分凝血活素时间(aPTT)将患者分为两组:高抗凝(AC)组(aPTT,≥55秒;n=52)和低ac组(aPTT)。结果:我们确定了10例出血患者;高ac组患者(n=8)明显多于低ac组(15.4% vs. 2.5%, p=0.01)。然而,血栓事件和氧合器无变化时间在两组之间无显著差异。高ac组4例患者死于出血并发症(脑出血2例;心包积血,1;还有胃肠道出血,其中之一)。低ac组中有1例患者发生血栓,并因电路血栓形成而死于ECMO功能障碍。结论:肝素不能显著改善血栓结局。然而,维持aPTT≥55秒是出血事件的重要危险因素,特别是与死亡率相关的出血事件。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
