Samer S Al-Droubi, Eiman Jahangir, Karl M Kochendorfer, Marianna Krive, Michal Laufer-Perl, Dan Gilon, Tochukwu M Okwuosa, Christopher P Gans, Joshua H Arnold, Shakthi T Bhaskar, Hesham A Yasin, Jacob Krive
{"title":"Artificial intelligence modelling to assess the risk of cardiovascular disease in oncology patients.","authors":"Samer S Al-Droubi, Eiman Jahangir, Karl M Kochendorfer, Marianna Krive, Michal Laufer-Perl, Dan Gilon, Tochukwu M Okwuosa, Christopher P Gans, Joshua H Arnold, Shakthi T Bhaskar, Hesham A Yasin, Jacob Krive","doi":"10.1093/ehjdh/ztad031","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>There are no comprehensive machine learning (ML) tools used by oncologists to assist with risk identification and referrals to cardio-oncology. This study applies ML algorithms to identify oncology patients at risk for cardiovascular disease for referrals to cardio-oncology and to generate risk scores to support quality of care.</p><p><strong>Methods and results: </strong>De-identified patient data were obtained from Vanderbilt University Medical Center. Patients with breast, kidney, and B-cell lymphoma cancers were targeted. Additionally, the study included patients who received immunotherapy drugs for treatment of melanoma, lung cancer, or kidney cancer. Random forest (RF) and artificial neural network (ANN) ML models were applied to analyse each cohort: A total of 20 023 records were analysed (breast cancer, 6299; B-cell lymphoma, 9227; kidney cancer, 2047; and immunotherapy for three covered cancers, 2450). Data were divided randomly into training (80%) and test (20%) data sets. Random forest and ANN performed over 90% for accuracy and area under the curve (AUC). All ANN models performed better than RF models and produced accurate referrals.</p><p><strong>Conclusion: </strong>Predictive models are ready for translation into oncology practice to identify and care for patients who are at risk of cardiovascular disease. The models are being integrated with electronic health record application as a report of patients who should be referred to cardio-oncology for monitoring and/or tailored treatments. Models operationally support cardio-oncology practice. Limited validation identified 86% of the lymphoma and 58% of the kidney cancer patients with major risk for cardiotoxicity who were not referred to cardio-oncology.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"4 4","pages":"302-315"},"PeriodicalIF":4.4000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5c/4d/ztad031.PMC10393891.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztad031","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Aims: There are no comprehensive machine learning (ML) tools used by oncologists to assist with risk identification and referrals to cardio-oncology. This study applies ML algorithms to identify oncology patients at risk for cardiovascular disease for referrals to cardio-oncology and to generate risk scores to support quality of care.
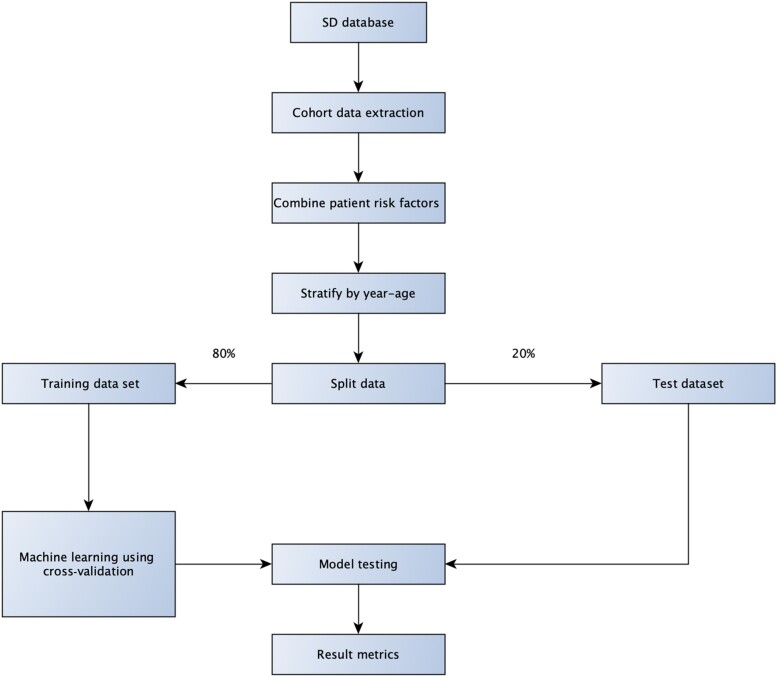
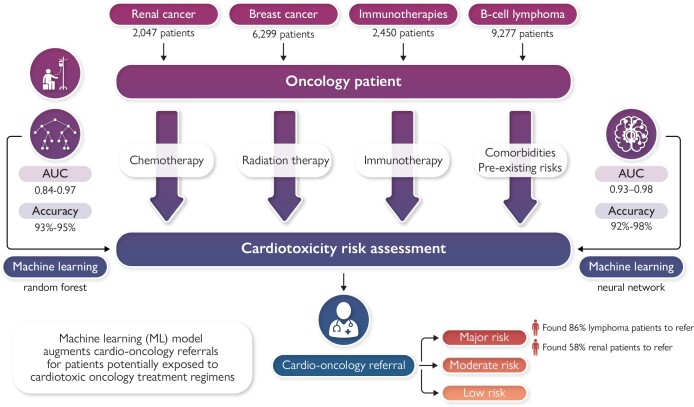
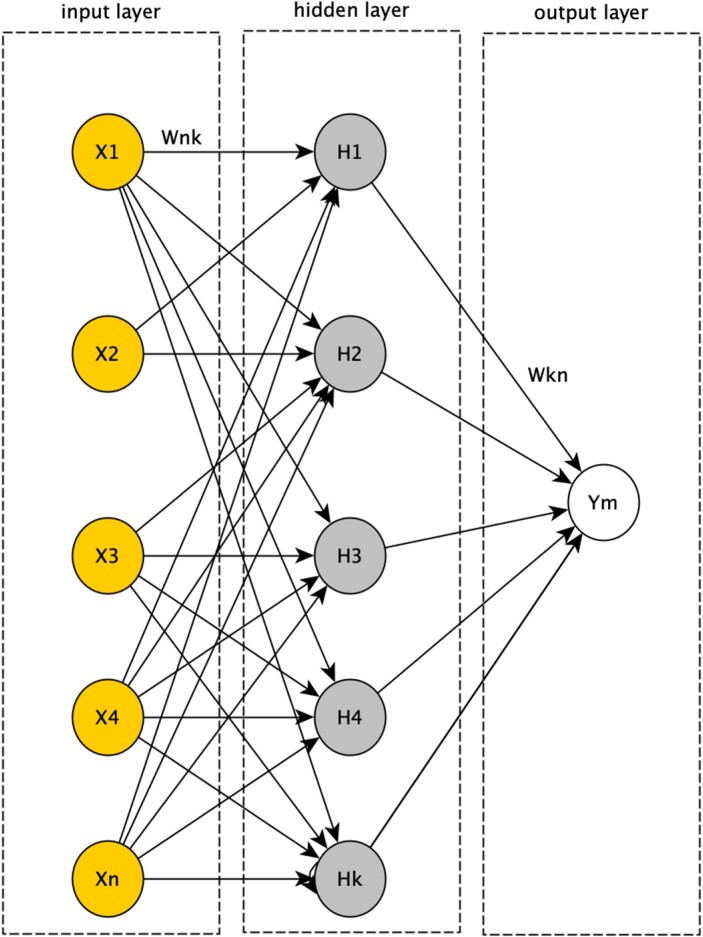
Methods and results: De-identified patient data were obtained from Vanderbilt University Medical Center. Patients with breast, kidney, and B-cell lymphoma cancers were targeted. Additionally, the study included patients who received immunotherapy drugs for treatment of melanoma, lung cancer, or kidney cancer. Random forest (RF) and artificial neural network (ANN) ML models were applied to analyse each cohort: A total of 20 023 records were analysed (breast cancer, 6299; B-cell lymphoma, 9227; kidney cancer, 2047; and immunotherapy for three covered cancers, 2450). Data were divided randomly into training (80%) and test (20%) data sets. Random forest and ANN performed over 90% for accuracy and area under the curve (AUC). All ANN models performed better than RF models and produced accurate referrals.
Conclusion: Predictive models are ready for translation into oncology practice to identify and care for patients who are at risk of cardiovascular disease. The models are being integrated with electronic health record application as a report of patients who should be referred to cardio-oncology for monitoring and/or tailored treatments. Models operationally support cardio-oncology practice. Limited validation identified 86% of the lymphoma and 58% of the kidney cancer patients with major risk for cardiotoxicity who were not referred to cardio-oncology.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
