{"title":"Variables affecting mortality rates in patients undergoing emergency abdominal surgery: A retrospective cross-sectional study.","authors":"Necmiye Ay, Abdurrahim Derbent, Ayça Sultan Şahin, Naime Yalcin, Mine Çelik","doi":"10.14744/tjtes.2022.01264","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients operated under emergency conditions have a higher risk of death and complications than those per-formed under elective conditions. Especially the patient group with high comorbidity needs to be evaluated more specifically. Accord-ing to the surgical risk and American Society of Anesthesiologists (ASA) scoring, the perioperative risk should be determined quickly, and the relatives of the patients should be informed. This study aimed to evaluate the factors affecting mortality and morbidity in patients undergoing emergency abdominal surgery.</p><p><strong>Methods: </strong>A total of 1065 patients aged 18 years and older who underwent emergency abdominal surgery in 1 year were included in the study. The primary aim of this study was to determine the mortality rates in the first 30 days and 1 year and the variables af-fecting these rates.</p><p><strong>Results: </strong>Of 1065 patients, 385 (36.2%) were female and 680 (63.8%) were male. The most common procedure was appendectomy (70.8%), followed by diagnostic laparotomy (10.2%), peptic ulcus perforation (6.7%), herniography (5.5%), colon resection (3.6%), and small bowel resection (3.2%). There was a significant difference between the age of the patients and mortality (p<0.05). There is no statistically significant relationship between gender and mortality. A statistically significant correlation was found between ASA scores, perioperative complication, perioperative blood product use, reoperation, intensive care unit admission, hospitalization time, periop-erative complication, and 30-day mortality and 1-year mortality. There is a significant relationship between trauma and only 30-day mortality (p=0.030).</p><p><strong>Conclusion: </strong>The morbidity and mortality of patients operated on under emergency conditions increased compared to elective surgical operations, especially those over age 70. The 30-day mortality rate of patients who underwent emergency abdominal surgery is 3%, while the 1-year mortality rate is 5.5%. Mortality rates are higher in patients with a high ASA risk score. However, mortality rates in our study were found to be higher than the mortality rates in ASA risk scoring.</p>","PeriodicalId":49398,"journal":{"name":"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery","volume":"29 4","pages":"505-513"},"PeriodicalIF":0.8000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/19/97/TJTES-29-505.PMC10214885.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14744/tjtes.2022.01264","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients operated under emergency conditions have a higher risk of death and complications than those per-formed under elective conditions. Especially the patient group with high comorbidity needs to be evaluated more specifically. Accord-ing to the surgical risk and American Society of Anesthesiologists (ASA) scoring, the perioperative risk should be determined quickly, and the relatives of the patients should be informed. This study aimed to evaluate the factors affecting mortality and morbidity in patients undergoing emergency abdominal surgery.
Methods: A total of 1065 patients aged 18 years and older who underwent emergency abdominal surgery in 1 year were included in the study. The primary aim of this study was to determine the mortality rates in the first 30 days and 1 year and the variables af-fecting these rates.
Results: Of 1065 patients, 385 (36.2%) were female and 680 (63.8%) were male. The most common procedure was appendectomy (70.8%), followed by diagnostic laparotomy (10.2%), peptic ulcus perforation (6.7%), herniography (5.5%), colon resection (3.6%), and small bowel resection (3.2%). There was a significant difference between the age of the patients and mortality (p<0.05). There is no statistically significant relationship between gender and mortality. A statistically significant correlation was found between ASA scores, perioperative complication, perioperative blood product use, reoperation, intensive care unit admission, hospitalization time, periop-erative complication, and 30-day mortality and 1-year mortality. There is a significant relationship between trauma and only 30-day mortality (p=0.030).
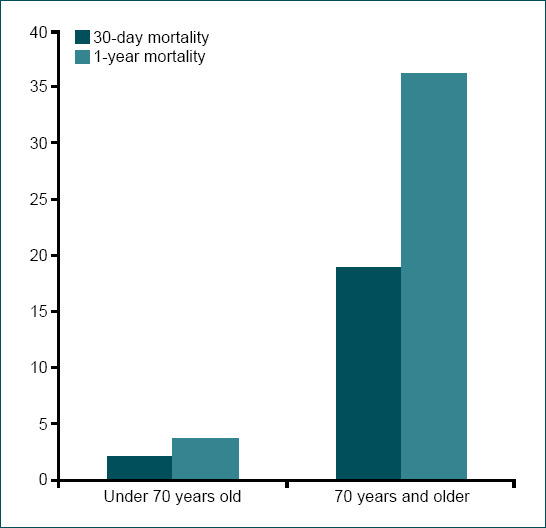
Conclusion: The morbidity and mortality of patients operated on under emergency conditions increased compared to elective surgical operations, especially those over age 70. The 30-day mortality rate of patients who underwent emergency abdominal surgery is 3%, while the 1-year mortality rate is 5.5%. Mortality rates are higher in patients with a high ASA risk score. However, mortality rates in our study were found to be higher than the mortality rates in ASA risk scoring.
期刊介绍:
The Turkish Journal of Trauma and Emergency Surgery (TJTES) is an official publication of the Turkish Association of Trauma and Emergency Surgery. It is a double-blind and peer-reviewed periodical that considers for publication clinical and experimental studies, case reports, technical contributions, and letters to the editor. Scope of the journal covers the trauma and emergency surgery.
Each submission will be reviewed by at least two external, independent peer reviewers who are experts in their fields in order to ensure an unbiased evaluation process. The editorial board will invite an external and independent reviewer to manage the evaluation processes of manuscripts submitted by editors or by the editorial board members of the journal. The Editor in Chief is the final authority in the decision-making process for all submissions.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
