{"title":"Impact of Pre-Transplant Parathyroidectomy on Graft Survival: A Comparative Study of Renal Transplant Patients (2005-2015).","authors":"Ming-Hsien Tsai, Mingchih Chen, Hung-Hsiang Liou, Tian-Shyug Lee, Yen-Chun Huang, Pei-Yang Liu, Yu-Wei Fang","doi":"10.12659/MSM.940959","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Hyperparathyroidism poses significant risks for patients prior to kidney transplantation. However, the outcomes of patients who undergo parathyroidectomy before renal transplantation compared to those without such a procedure remain uncertain. This real-world data study aimed to examine the clinical outcomes of both patient groups. MATERIAL AND METHODS Using the Taiwan National Health Insurance Research Database, we conducted a retrospective cohort study on patients who underwent renal transplantation between January 2005 and December 2015. The patients were divided into two groups: a case group (n=294) with parathyroidectomy and a control group (n=588) without the need for parathyroidectomy before kidney transplantation. The groups were matched based on age, sex, dialysis vintage, and baseline characteristics at a 1:2 ratio. Hazard ratios (HR) were estimated using the Cox regression model. The main outcomes assessed were graft failure, mortality, and major adverse cardiovascular events (MACE) recorded until December 2019. RESULTS During a mean follow-up period of 6 years, a significant difference was observed in graft failure (HR 1.40; 95% confidence interval 1.10-1.79, p=0.007) between the two groups. After further adjustment, graft failure remained significant (HR 1.52; 95% CI 1.07-2.15, p=0.019). Additionally, machine learning-based feature selection identified the importance of parathyroidectomy (ranked 9 out of 11) before kidney transplantation in predicting subsequent graft failure. CONCLUSIONS Our study demonstrates that severe hyperparathyroidism requiring parathyroidectomy before kidney transplantation may contribute to poor post-transplant graft outcomes compared to patients who do not require parathyroidectomy.</p>","PeriodicalId":18276,"journal":{"name":"Medical Science Monitor : International Medical Journal of Experimental and Clinical Research","volume":"29 ","pages":"e940959"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e1/db/medscimonit-29-e940959.PMC10403992.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Science Monitor : International Medical Journal of Experimental and Clinical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/MSM.940959","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
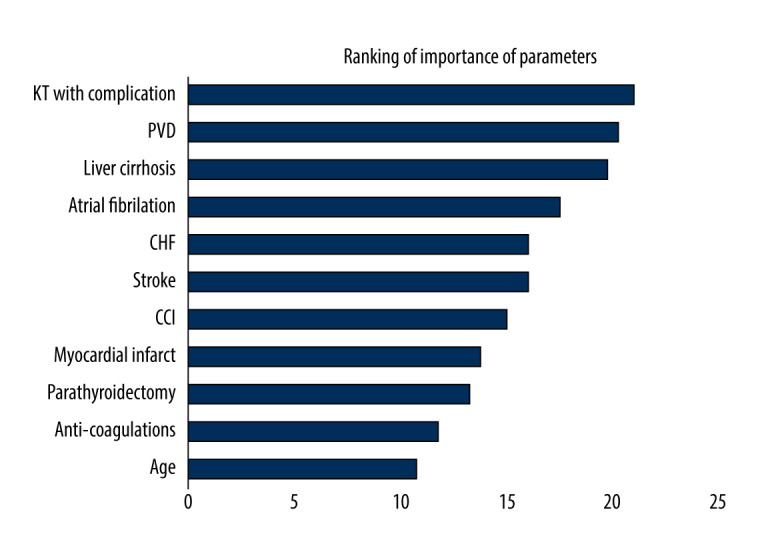
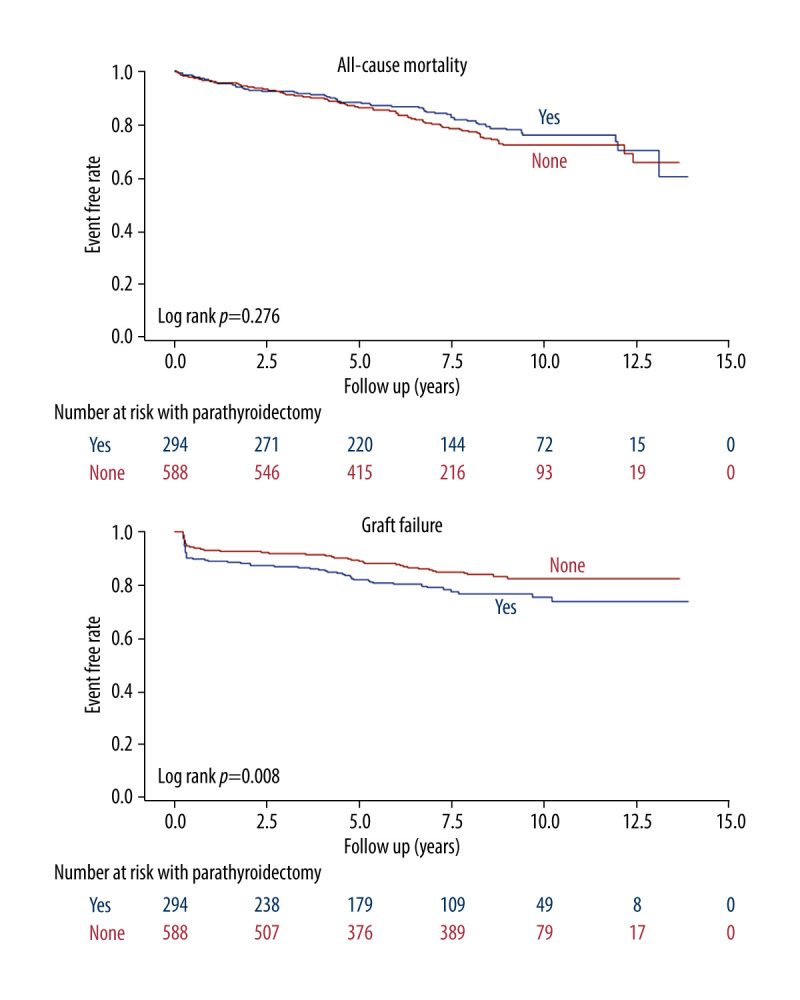
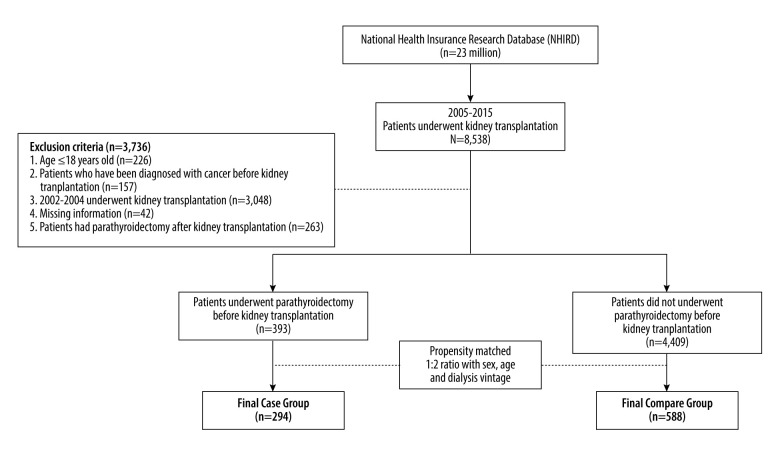
BACKGROUND Hyperparathyroidism poses significant risks for patients prior to kidney transplantation. However, the outcomes of patients who undergo parathyroidectomy before renal transplantation compared to those without such a procedure remain uncertain. This real-world data study aimed to examine the clinical outcomes of both patient groups. MATERIAL AND METHODS Using the Taiwan National Health Insurance Research Database, we conducted a retrospective cohort study on patients who underwent renal transplantation between January 2005 and December 2015. The patients were divided into two groups: a case group (n=294) with parathyroidectomy and a control group (n=588) without the need for parathyroidectomy before kidney transplantation. The groups were matched based on age, sex, dialysis vintage, and baseline characteristics at a 1:2 ratio. Hazard ratios (HR) were estimated using the Cox regression model. The main outcomes assessed were graft failure, mortality, and major adverse cardiovascular events (MACE) recorded until December 2019. RESULTS During a mean follow-up period of 6 years, a significant difference was observed in graft failure (HR 1.40; 95% confidence interval 1.10-1.79, p=0.007) between the two groups. After further adjustment, graft failure remained significant (HR 1.52; 95% CI 1.07-2.15, p=0.019). Additionally, machine learning-based feature selection identified the importance of parathyroidectomy (ranked 9 out of 11) before kidney transplantation in predicting subsequent graft failure. CONCLUSIONS Our study demonstrates that severe hyperparathyroidism requiring parathyroidectomy before kidney transplantation may contribute to poor post-transplant graft outcomes compared to patients who do not require parathyroidectomy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
