Characteristics, Antithrombotic Patterns, and Prognostic Outcomes in Claudication and Critical Limb-Threatening Ischemia Undergoing Endovascular Therapy.
{"title":"Characteristics, Antithrombotic Patterns, and Prognostic Outcomes in Claudication and Critical Limb-Threatening Ischemia Undergoing Endovascular Therapy.","authors":"Osami Kawarada, Kan Zen, Koji Hozawa, Hideaki Obara, Kentaro Matsubara, Yoshito Yamamoto, Tatsuki Doijiri, Nozomu Tamai, Shigenori Ito, Akihiro Higashimori, Daizo Kawasaki, Hideki Doi, Kensuke Matsushita, Kengo Tsukahara, Katsuo Noda, Masahisa Shimpo, Yuki Tsuda, Shinjo Sonoda, Takuya Taniguchi, Katsuhisa Waseda, Masato Munehisa, Eiji Taguchi, Tatsuya Kinjo, Yohei Sasaki, Kenichiro Yuba, Shinichiro Yamaguchi, Takuo Nakagami, Shinobu Ayabe, Shingo Sakamoto, Takeshi Yagyu, Soshiro Ogata, Kunihiro Nishimura, Hisashi Motomura, Teruo Noguchi, Masaharu Ishihara, Hisao Ogawa, Satoshi Yasuda","doi":"10.1177/15266028221134886","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The underlying difference between intermittent claudication (IC) and critical limb-threatening ischemia (CLTI) still remains unclear. This prospective multicenter observational study aimed to clarify differences in clinical features and prognostic outcomes between IC and CLTI, and prognostic factors in patients undergoing endovascular therapy (EVT).</p><p><strong>Materials and methods: </strong>A total of 692 patients with 808 limbs were enrolled from 20 institutions in Japan. The primary measurements were the 3-year rates of major adverse cardiovascular event (MACE) and reintervention.</p><p><strong>Results: </strong>Among patients, 79.0% had IC and 21.0% had CLTI. Patients with CLTI were more frequently women and more likely to have impaired functional status, undernutrition, comorbidities, hypercoagulation, hyperinflammation, distal artery disease, short single antiplatelet and long anticoagulation therapies, and late cilostazol than patients with IC. Aortoiliac and femoropopliteal diseases were dominant in patients with IC and infrapopliteal disease was dominant in patients with CLTI. Patients with CLTI underwent less frequently aortoiliac intervention and more frequently infrapopliteal intervention than patients with IC. Longitudinal change of ankle-brachial index (ABI) exhibited different patterns between IC and CLTI (pinteraction=0.002), but ABI improved after EVT both in IC and in CLTI (p<0.001), which was sustained over time. Dorsal and plantar skin perfusion pressure in CLTI showed a similar improvement pattern (pinteraction=0.181). Distribution of Rutherford category improved both in IC and in CLTI (each p<0.001). Three-year MACE rates were 20.4% and 42.3% and 3-year reintervention rates were 22.1% and 46.8% for patients with IC and CLTI, respectively (log-rank p<0.001). Elevated D-dimer (p=0.001), age (p=0.043), impaired functional status (p=0.018), and end-stage renal disease (p=0.019) were independently associated with MACE. After considering competing risks of death and major amputation for reintervention, elevated erythrocyte sedimentation rate (p=0.003) and infrainguinal intervention (p=0.002) were independently associated with reintervention. Patients with CLTI merely showed borderline significance for MACE (adjusted hazard ratio 1.700, 95% confidence interval 0.950-3.042, p=0.074) and reintervention (adjusted hazard ratio 1.976, 95% confidence interval 0.999-3.909, p=0.05).</p><p><strong>Conclusions: </strong>The CLTI is characterized not only by more systemic comorbidities and distal disease but also by more inflammatory coagulation disorder compared with IC. Also, CLTI has approximately twice MACE and reintervention rates than IC, and the underlying inflammatory coagulation disorder per se is associated with these outcomes.</p><p><strong>Clinical impact: </strong>The underlying difference between intermittent claudication (IC) and critical limb-threatening ischemia (CLTI) still remains unclear. This prospective multicenter observational study, JPASSION study found that CLTI was characterized not only by more systemic comorbidities and distal disease but also by more inflammatory coagulation disorder compared to IC. Also, CLTI had approximately twice major adverse cardiovascular event (MACE) and reintervention rates than IC. Intriguingly, the underlying inflammatory coagulation disorder per se was independently associated with MACE and reintervention. Further studies to clarify the role of anticoagulation and anti-inflammatory therapies will contribute to the development of post-interventional therapeutics in the context of peripheral artery disease.</p>","PeriodicalId":50210,"journal":{"name":"Journal of Endovascular Therapy","volume":" ","pages":"622-633"},"PeriodicalIF":1.5000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11512489/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Endovascular Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/15266028221134886","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The underlying difference between intermittent claudication (IC) and critical limb-threatening ischemia (CLTI) still remains unclear. This prospective multicenter observational study aimed to clarify differences in clinical features and prognostic outcomes between IC and CLTI, and prognostic factors in patients undergoing endovascular therapy (EVT).
Materials and methods: A total of 692 patients with 808 limbs were enrolled from 20 institutions in Japan. The primary measurements were the 3-year rates of major adverse cardiovascular event (MACE) and reintervention.
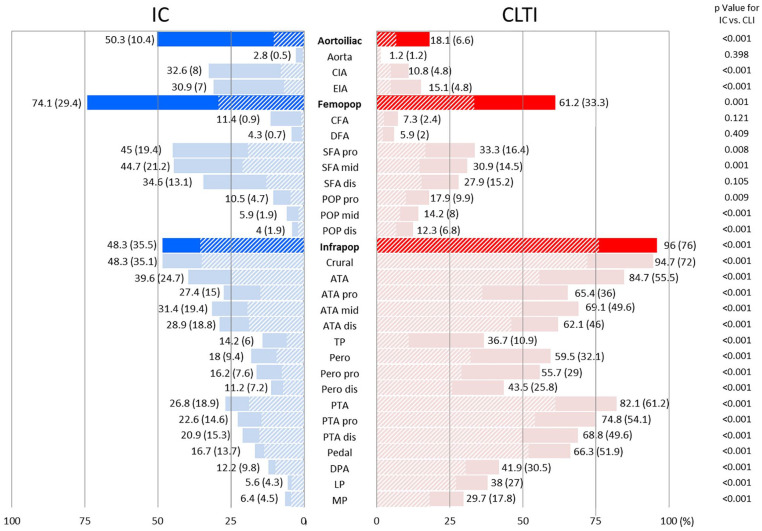
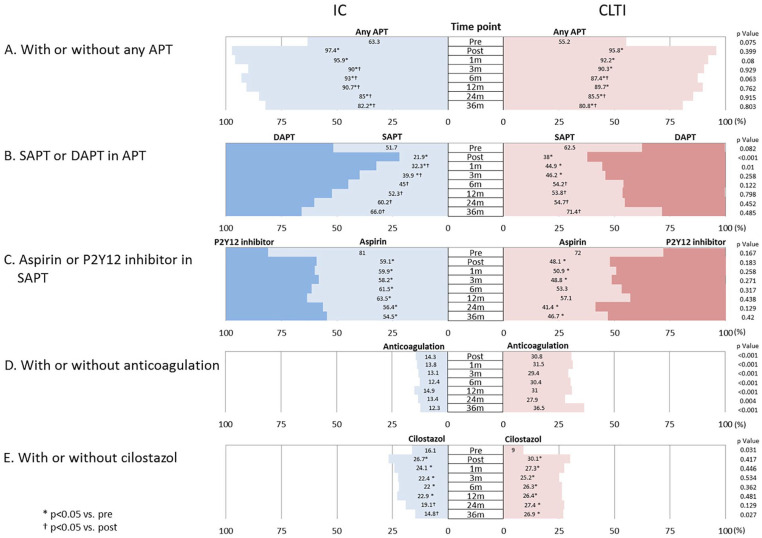
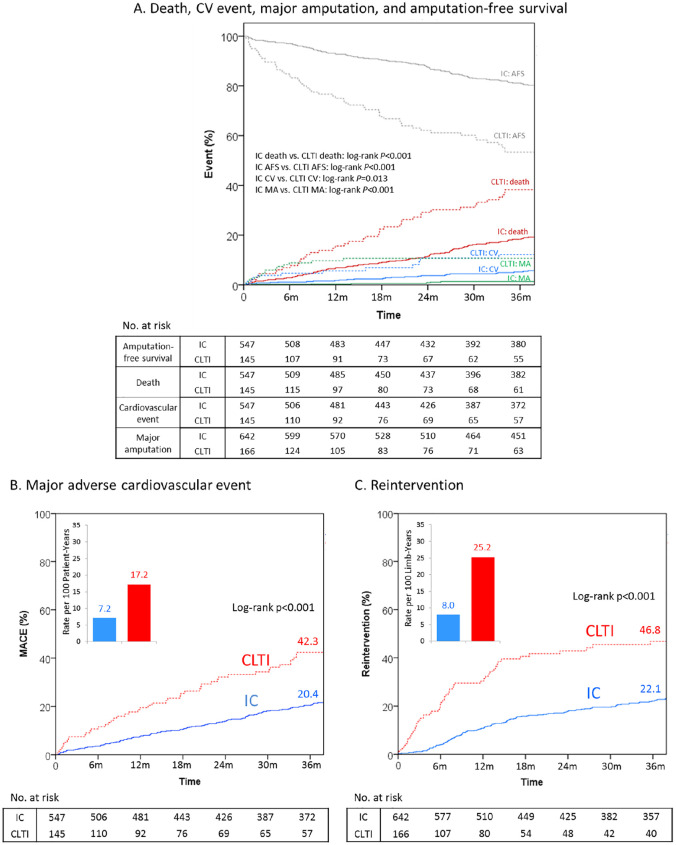
Results: Among patients, 79.0% had IC and 21.0% had CLTI. Patients with CLTI were more frequently women and more likely to have impaired functional status, undernutrition, comorbidities, hypercoagulation, hyperinflammation, distal artery disease, short single antiplatelet and long anticoagulation therapies, and late cilostazol than patients with IC. Aortoiliac and femoropopliteal diseases were dominant in patients with IC and infrapopliteal disease was dominant in patients with CLTI. Patients with CLTI underwent less frequently aortoiliac intervention and more frequently infrapopliteal intervention than patients with IC. Longitudinal change of ankle-brachial index (ABI) exhibited different patterns between IC and CLTI (pinteraction=0.002), but ABI improved after EVT both in IC and in CLTI (p<0.001), which was sustained over time. Dorsal and plantar skin perfusion pressure in CLTI showed a similar improvement pattern (pinteraction=0.181). Distribution of Rutherford category improved both in IC and in CLTI (each p<0.001). Three-year MACE rates were 20.4% and 42.3% and 3-year reintervention rates were 22.1% and 46.8% for patients with IC and CLTI, respectively (log-rank p<0.001). Elevated D-dimer (p=0.001), age (p=0.043), impaired functional status (p=0.018), and end-stage renal disease (p=0.019) were independently associated with MACE. After considering competing risks of death and major amputation for reintervention, elevated erythrocyte sedimentation rate (p=0.003) and infrainguinal intervention (p=0.002) were independently associated with reintervention. Patients with CLTI merely showed borderline significance for MACE (adjusted hazard ratio 1.700, 95% confidence interval 0.950-3.042, p=0.074) and reintervention (adjusted hazard ratio 1.976, 95% confidence interval 0.999-3.909, p=0.05).
Conclusions: The CLTI is characterized not only by more systemic comorbidities and distal disease but also by more inflammatory coagulation disorder compared with IC. Also, CLTI has approximately twice MACE and reintervention rates than IC, and the underlying inflammatory coagulation disorder per se is associated with these outcomes.
Clinical impact: The underlying difference between intermittent claudication (IC) and critical limb-threatening ischemia (CLTI) still remains unclear. This prospective multicenter observational study, JPASSION study found that CLTI was characterized not only by more systemic comorbidities and distal disease but also by more inflammatory coagulation disorder compared to IC. Also, CLTI had approximately twice major adverse cardiovascular event (MACE) and reintervention rates than IC. Intriguingly, the underlying inflammatory coagulation disorder per se was independently associated with MACE and reintervention. Further studies to clarify the role of anticoagulation and anti-inflammatory therapies will contribute to the development of post-interventional therapeutics in the context of peripheral artery disease.
期刊介绍:
The Journal of Endovascular Therapy (formerly the Journal of Endovascular Surgery) was established in 1994 as a forum for all physicians, scientists, and allied healthcare professionals who are engaged or interested in peripheral endovascular techniques and technology. An official publication of the International Society of Endovascular Specialists (ISEVS), the Journal of Endovascular Therapy publishes peer-reviewed articles of interest to clinicians and researchers in the field of peripheral endovascular interventions.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
