Tatiana Baglo, Alban Gildas Comlan Zohoun, Lutécia Zohoun, Antoine Sianou, Dorothée Kindé Gazard
{"title":"[Influence of white blood cells count on parasite density in Malaria in children aged 6 to 59 months in Benin].","authors":"Tatiana Baglo, Alban Gildas Comlan Zohoun, Lutécia Zohoun, Antoine Sianou, Dorothée Kindé Gazard","doi":"10.48327/mtsi.v3i2.2023.321","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>For many years, the treatment of malaria was based on clinical presumptive diagnosis, making its differential diagnosis with other causes of hyperthermia difficult. This drug pressure has led to the emergence of <i>Plasmodium</i> strains resistant to the most commonly used antimalarial drugs. This is why in 2004, the health authorities decided to revise the policy of malaria management by adopting a new strategy based on the rational use of artemisininbased combination therapies after the biological confirmation of suspected malaria cases. The biological diagnosis is an essential part of malaria management. The gold standard technique for diagnosis is the thick drop combined with the calculation of parasite density (PD), which is determined on the basis of the number of parasites counted in a microscopic field against a proposed standard number of leukocytes. The number of leukocytes used to calculate the parasite density should ideally be the actual number of leukocytes in the patient per cubic millimetre of blood. However, in the absence of the availability of a blood count at the time of the thick drop, an average number of 8 000 leukocytes/mm<sup>3</sup> was used by the World Health Organisation (WHO) to estimate the parasite density. Nonetheless, in Benin the average number of leukocytes adopted by the National Malaria Control Programme (PNLP) is 6 000/mm<sup>3</sup>. The aim of our study was to determine the impact of the leukocyte count on the calculation of the parasite density in cases of uncomplicated malaria.</p><p><strong>Method: </strong>The study was a cross-sectional study with an analytical aim and took place in 2 hospitals in Benin, the Klouékanmey zone hospital in the south of Benin and the Djougou health centre in the north. It involved a population of 476 children aged between 6 and 59 months who were seen in consultation and in whom the clinical diagnosis of simple <i>Plasmodium falciparum</i> malaria was suspected. Children aged between 6 and 59 months, weighing at least 5 kg, with an axillary temperature ≥ 37.5°C at the time of consultation or a history of fever in the last 24 hours or other symptoms pointing to the diagnosis of malaria were included. Infestation was mono-specific for <i>Plasmodium falciparum.</i> Informed consent was required from the child's parents or guardian. The criteria for non-inclusion in our study were the presence of at least one sign of malaria severity, signs of severe malnutrition or a febrile state related to underlying infectious diseases other than malaria. Thick blood count and haemogram were systematically performed in all included children. Parasite density was calculated according to 3 methods, first using a weighted leukocyte count of 6 000/mm<sup>3</sup> recommended by the Benin National Malaria Control Programme (PNLP), then a leukocyte count of 8 000/mm<sup>3</sup> recommended by the World Health Organisation and finally the patient's actual leukocyte count obtained from the blood count. It should be noted that these different samples were respectively taken on the day of inclusion in compliance with the conditions of the pre-analytical phase in force in our medical biology laboratory.</p><p><strong>Results: </strong>At the end of our study, 313 children, i.e. 65.76% of our study population had a positive white blood cell count with a positivity rate of 62.14% in Djougou, i.e. 174 children, and 70.9% in Klouékanmey, i.e. 139 children. The average leukocyte count in these children was 11,580/mm<sup>3</sup>. Among them, 205 children had an abnormal white blood cell count, i.e. 17 cases of leukopenia (5.43%) and 188 cases of hyperleukocytosis (60.06%). Using successively the average number of 6 000 leukocytes/mm<sup>3</sup> proposed by the Benin PNLP and that of 8 000 leukocytes/mm<sup>3</sup> proposed by the WHO, the average parasite densities were respectively 47,943 and 63,936 trophozoïtes/µl against 92,290 trophozoïtes/µl when the real number of leukocytes of the patients was used for the calculation of the PD. By using an average of 6 000 leukocytes/mm<sup>3</sup> for PD calculation, 60% of the calculated PDs were underestimated and 6% were overestimated. Using an average of 8 000 leukocytes/mm<sup>3</sup> resulted in 49% of PD being underestimated and 15% being overestimated. The difference between the three calculation methods was considered statistically significant (p value <0.05).</p><p><strong>Conclusion: </strong>The use of 6 000 or 8 000 coefficients for the estimation of parasitaemia could lead to a significant underestimation of the parasite load.</p>","PeriodicalId":18493,"journal":{"name":"Medecine tropicale et sante internationale","volume":"3 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10387309/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medecine tropicale et sante internationale","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.48327/mtsi.v3i2.2023.321","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: For many years, the treatment of malaria was based on clinical presumptive diagnosis, making its differential diagnosis with other causes of hyperthermia difficult. This drug pressure has led to the emergence of Plasmodium strains resistant to the most commonly used antimalarial drugs. This is why in 2004, the health authorities decided to revise the policy of malaria management by adopting a new strategy based on the rational use of artemisininbased combination therapies after the biological confirmation of suspected malaria cases. The biological diagnosis is an essential part of malaria management. The gold standard technique for diagnosis is the thick drop combined with the calculation of parasite density (PD), which is determined on the basis of the number of parasites counted in a microscopic field against a proposed standard number of leukocytes. The number of leukocytes used to calculate the parasite density should ideally be the actual number of leukocytes in the patient per cubic millimetre of blood. However, in the absence of the availability of a blood count at the time of the thick drop, an average number of 8 000 leukocytes/mm3 was used by the World Health Organisation (WHO) to estimate the parasite density. Nonetheless, in Benin the average number of leukocytes adopted by the National Malaria Control Programme (PNLP) is 6 000/mm3. The aim of our study was to determine the impact of the leukocyte count on the calculation of the parasite density in cases of uncomplicated malaria.
Method: The study was a cross-sectional study with an analytical aim and took place in 2 hospitals in Benin, the Klouékanmey zone hospital in the south of Benin and the Djougou health centre in the north. It involved a population of 476 children aged between 6 and 59 months who were seen in consultation and in whom the clinical diagnosis of simple Plasmodium falciparum malaria was suspected. Children aged between 6 and 59 months, weighing at least 5 kg, with an axillary temperature ≥ 37.5°C at the time of consultation or a history of fever in the last 24 hours or other symptoms pointing to the diagnosis of malaria were included. Infestation was mono-specific for Plasmodium falciparum. Informed consent was required from the child's parents or guardian. The criteria for non-inclusion in our study were the presence of at least one sign of malaria severity, signs of severe malnutrition or a febrile state related to underlying infectious diseases other than malaria. Thick blood count and haemogram were systematically performed in all included children. Parasite density was calculated according to 3 methods, first using a weighted leukocyte count of 6 000/mm3 recommended by the Benin National Malaria Control Programme (PNLP), then a leukocyte count of 8 000/mm3 recommended by the World Health Organisation and finally the patient's actual leukocyte count obtained from the blood count. It should be noted that these different samples were respectively taken on the day of inclusion in compliance with the conditions of the pre-analytical phase in force in our medical biology laboratory.
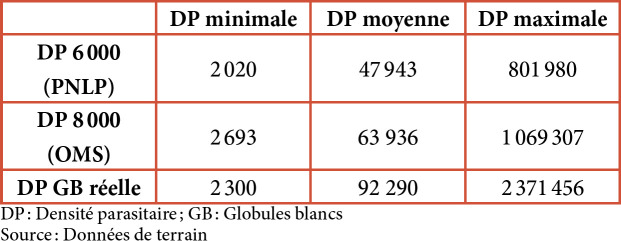
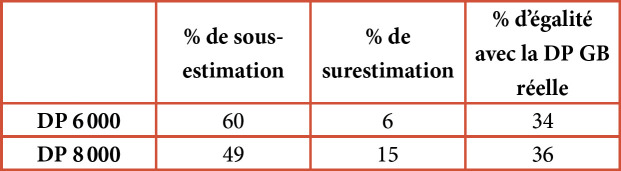
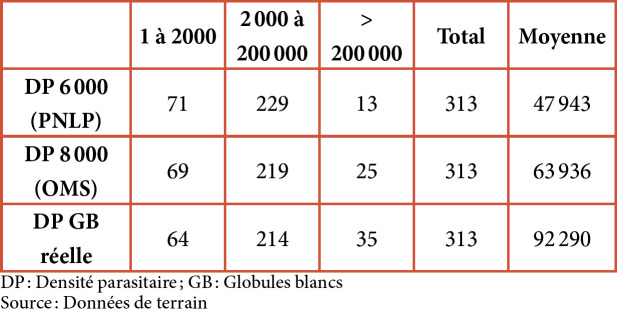
Results: At the end of our study, 313 children, i.e. 65.76% of our study population had a positive white blood cell count with a positivity rate of 62.14% in Djougou, i.e. 174 children, and 70.9% in Klouékanmey, i.e. 139 children. The average leukocyte count in these children was 11,580/mm3. Among them, 205 children had an abnormal white blood cell count, i.e. 17 cases of leukopenia (5.43%) and 188 cases of hyperleukocytosis (60.06%). Using successively the average number of 6 000 leukocytes/mm3 proposed by the Benin PNLP and that of 8 000 leukocytes/mm3 proposed by the WHO, the average parasite densities were respectively 47,943 and 63,936 trophozoïtes/µl against 92,290 trophozoïtes/µl when the real number of leukocytes of the patients was used for the calculation of the PD. By using an average of 6 000 leukocytes/mm3 for PD calculation, 60% of the calculated PDs were underestimated and 6% were overestimated. Using an average of 8 000 leukocytes/mm3 resulted in 49% of PD being underestimated and 15% being overestimated. The difference between the three calculation methods was considered statistically significant (p value <0.05).
Conclusion: The use of 6 000 or 8 000 coefficients for the estimation of parasitaemia could lead to a significant underestimation of the parasite load.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
