Thomas Newman, Raunak Borker, Louise Aubiniere-Robb, Justin Hendrickson, Dipankar Choudhury, Ian Halliday, John Fenner, Andrew Narracott, D Rodney Hose, Rebecca Gosling, Julian P Gunn, Paul D Morris
{"title":"Rapid virtual fractional flow reserve using 3D computational fluid dynamics.","authors":"Thomas Newman, Raunak Borker, Louise Aubiniere-Robb, Justin Hendrickson, Dipankar Choudhury, Ian Halliday, John Fenner, Andrew Narracott, D Rodney Hose, Rebecca Gosling, Julian P Gunn, Paul D Morris","doi":"10.1093/ehjdh/ztad028","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Over the last ten years, virtual Fractional Flow Reserve (vFFR) has improved the utility of Fractional Flow Reserve (FFR), a globally recommended assessment to guide coronary interventions. Although the speed of vFFR computation has accelerated, techniques utilising full 3D computational fluid dynamics (CFD) solutions rather than simplified analytical solutions still require significant time to compute.</p><p><strong>Methods and results: </strong>This study investigated the speed, accuracy and cost of a novel 3D-CFD software method based upon a graphic processing unit (GPU) computation, compared with the existing fastest central processing unit (CPU)-based 3D-CFD technique, on 40 angiographic cases. The novel GPU simulation was significantly faster than the CPU method (median 31.7 s (Interquartile Range (IQR) 24.0-44.4s) vs. 607.5 s (490-964 s), <i>P</i> < 0.0001). The novel GPU technique was 99.6% (IQR 99.3-99.9) accurate relative to the CPU method. The initial cost of the GPU hardware was greater than the CPU (£4080 vs. £2876), but the median energy consumption per case was significantly less using the GPU method (8.44 (6.80-13.39) Wh vs. 2.60 (2.16-3.12) Wh, <i>P</i> < 0.0001).</p><p><strong>Conclusion: </strong>This study demonstrates that vFFR can be computed using 3D-CFD with up to 28-fold acceleration than previous techniques with no clinically significant sacrifice in accuracy.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"4 4","pages":"283-290"},"PeriodicalIF":4.4000,"publicationDate":"2023-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10393878/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztad028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
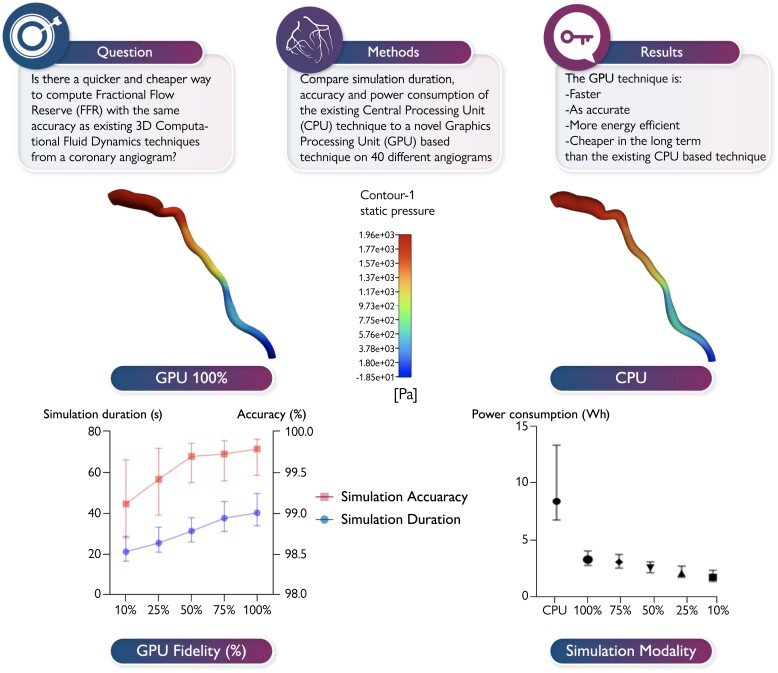
Aims: Over the last ten years, virtual Fractional Flow Reserve (vFFR) has improved the utility of Fractional Flow Reserve (FFR), a globally recommended assessment to guide coronary interventions. Although the speed of vFFR computation has accelerated, techniques utilising full 3D computational fluid dynamics (CFD) solutions rather than simplified analytical solutions still require significant time to compute.
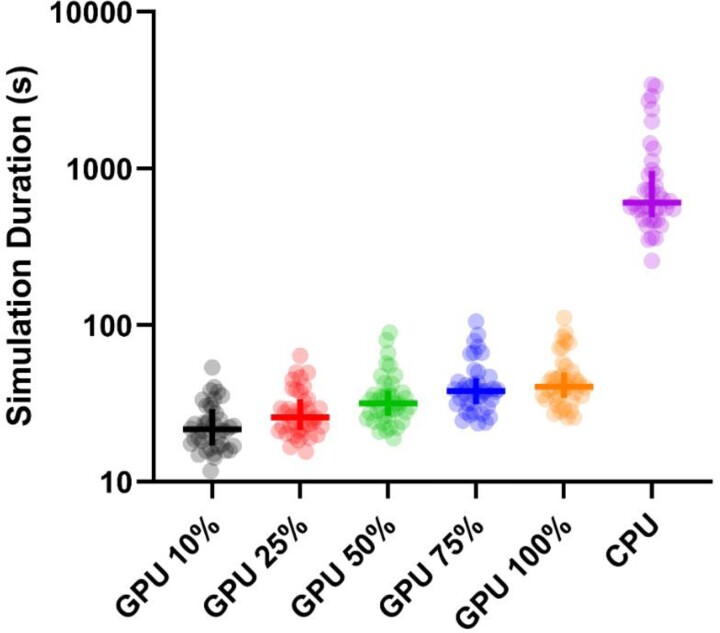
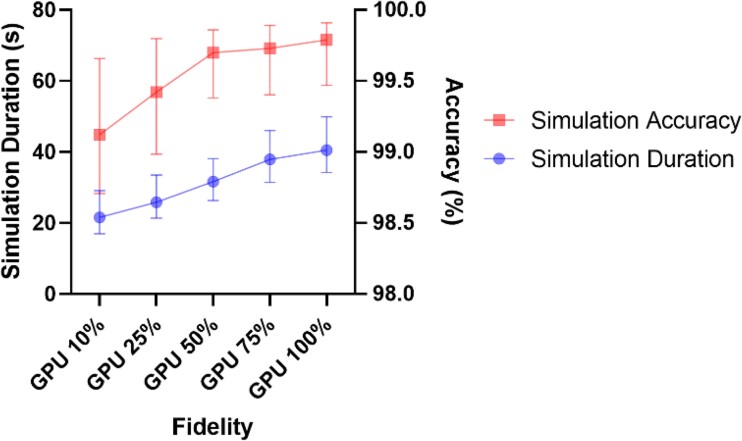
Methods and results: This study investigated the speed, accuracy and cost of a novel 3D-CFD software method based upon a graphic processing unit (GPU) computation, compared with the existing fastest central processing unit (CPU)-based 3D-CFD technique, on 40 angiographic cases. The novel GPU simulation was significantly faster than the CPU method (median 31.7 s (Interquartile Range (IQR) 24.0-44.4s) vs. 607.5 s (490-964 s), P < 0.0001). The novel GPU technique was 99.6% (IQR 99.3-99.9) accurate relative to the CPU method. The initial cost of the GPU hardware was greater than the CPU (£4080 vs. £2876), but the median energy consumption per case was significantly less using the GPU method (8.44 (6.80-13.39) Wh vs. 2.60 (2.16-3.12) Wh, P < 0.0001).
Conclusion: This study demonstrates that vFFR can be computed using 3D-CFD with up to 28-fold acceleration than previous techniques with no clinically significant sacrifice in accuracy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
