{"title":"Pharmacotherapy treatment patterns at hospital discharge and clinical outcomes among patients with heart failure with reduced ejection fraction","authors":"Yuttana Wongsalap, Duangkamon Poolpun, Konrapee Keawhai, Napusson Kitpluem, Parichat Pansiri, Siriluck Malaimat, Vichai Senthong, Kirati Kengkla","doi":"10.1002/cdt3.59","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>This study aimed to assess the prescribing patterns of evidence-based pharmacotherapy and their association with clinical outcomes in patients with heart failure with reduced ejection fraction (HFrEF) in Thailand.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A retrospective cohort study of patients with HFrEF was conducted. Treatment with a β-blocker and renin–angiotensin system inhibitors (RASIs) with or without mineralocorticoid receptor antagonists (MRAs) at discharge was regarded as guideline-directed medical therapy (GDMT). All others were considered non-GDMT. The primary endpoint was the composite of all-cause mortality or heart failure (HF) rehospitalization. Inverse-probability-treatment-weighted adjusted Cox proportional hazard models were used to examine the treatment effects.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In total, 653 patients with HFrEF (mean age 64.1 ± 14.3 years; 55.9% male) were included. GDMT with β-blockers and RASIs with or without MRAs was prescribed at a rate of 35.4%. During a median of 1-year follow-up, 167 patients (27.5%) had a composite event, 81 patients (13.3%) had all-cause mortality, and 109 patients (18.0%) had HF rehospitalization. Patients treated with GDMT at discharge showed significantly lower rates of the primary endpoint (adjusted hazard ratio [HR] 0.63; 95% CI 0.44–0.89; <i>p</i> = 0.009) compared with patients who did not receive GDMT. The use of GDMT was also associated with a significantly lower risk of all-cause mortality (adjusted HR 0.59; 95% CI 0.36–0.98; <i>p</i> = 0.045) and HF rehospitalization (adjusted HR 0.65; 95% CI 0.43–0.96; <i>p</i> = 0.031).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>For HFrEF treatment, GDMT initiation at hospital discharge was associated with a significantly reduced risk of all-cause mortality and HF rehospitalization. Nevertheless, prescribing GDMT remains underused, and it could be encouraged to improve HF outcomes in real-world settings.</p>\n </section>\n </div>","PeriodicalId":32096,"journal":{"name":"Chronic Diseases and Translational Medicine","volume":"9 2","pages":"154-163"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/65/e9/CDT3-9-154.PMC10249177.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Diseases and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.59","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background
This study aimed to assess the prescribing patterns of evidence-based pharmacotherapy and their association with clinical outcomes in patients with heart failure with reduced ejection fraction (HFrEF) in Thailand.
Methods
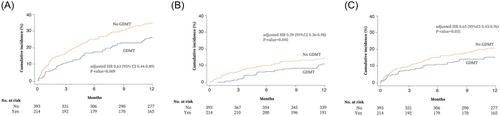
A retrospective cohort study of patients with HFrEF was conducted. Treatment with a β-blocker and renin–angiotensin system inhibitors (RASIs) with or without mineralocorticoid receptor antagonists (MRAs) at discharge was regarded as guideline-directed medical therapy (GDMT). All others were considered non-GDMT. The primary endpoint was the composite of all-cause mortality or heart failure (HF) rehospitalization. Inverse-probability-treatment-weighted adjusted Cox proportional hazard models were used to examine the treatment effects.
Results
In total, 653 patients with HFrEF (mean age 64.1 ± 14.3 years; 55.9% male) were included. GDMT with β-blockers and RASIs with or without MRAs was prescribed at a rate of 35.4%. During a median of 1-year follow-up, 167 patients (27.5%) had a composite event, 81 patients (13.3%) had all-cause mortality, and 109 patients (18.0%) had HF rehospitalization. Patients treated with GDMT at discharge showed significantly lower rates of the primary endpoint (adjusted hazard ratio [HR] 0.63; 95% CI 0.44–0.89; p = 0.009) compared with patients who did not receive GDMT. The use of GDMT was also associated with a significantly lower risk of all-cause mortality (adjusted HR 0.59; 95% CI 0.36–0.98; p = 0.045) and HF rehospitalization (adjusted HR 0.65; 95% CI 0.43–0.96; p = 0.031).
Conclusions
For HFrEF treatment, GDMT initiation at hospital discharge was associated with a significantly reduced risk of all-cause mortality and HF rehospitalization. Nevertheless, prescribing GDMT remains underused, and it could be encouraged to improve HF outcomes in real-world settings.
期刊介绍:
This journal aims to promote progress from basic research to clinical practice and to provide a forum for communication among basic, translational, and clinical research practitioners and physicians from all relevant disciplines. Chronic diseases such as cardiovascular diseases, cancer, diabetes, stroke, chronic respiratory diseases (such as asthma and COPD), chronic kidney diseases, and related translational research. Topics of interest for Chronic Diseases and Translational Medicine include Research and commentary on models of chronic diseases with significant implications for disease diagnosis and treatment Investigative studies of human biology with an emphasis on disease Perspectives and reviews on research topics that discuss the implications of findings from the viewpoints of basic science and clinical practic.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
