Pregnancy outcomes in women with adenomyosis, undergoing artificial endometrial preparation with and without gonadotropin-releasing hormone agonist pretreatment in frozen embryo transfer cycles: An RCT.
{"title":"Pregnancy outcomes in women with adenomyosis, undergoing artificial endometrial preparation with and without gonadotropin-releasing hormone agonist pretreatment in frozen embryo transfer cycles: An RCT.","authors":"Marzieh Eslami Moayed, Ashraf Moini, Ladan Kashani, Maryam Farid Mojtahedi, Tawoos Rezaee, Hamed Tabasizadeh, Khadije Maajani, Nazila Yamini","doi":"10.18502/ijrm.v21i6.13635","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Selecting a suitable and preferable method for endometrial preparation in frozen embryo transfer (FET) cycles for women with adenomyosis is still challenging in infertility treatment.</p><p><strong>Objective: </strong>To compare 2 artificial endometrial preparation regimens with and without gonadotropin-releasing hormone agonist (GnRHa) pretreatment in women with adenomyosis undergoing FET cycles.</p><p><strong>Materials and methods: </strong>This randomized clinical trial study was conducted on 140 adenomyosis cases who underwent FET cycles at Arash Women's hospital, Tehran, Iran from May 2020 to March 2021. Participants were randomly allocated into hormonal replacement therapy (HRT) and HRT+GnRHa pretreatment groups (n = 70/each). Endometrial preparation with 2-6 mg daily estradiol was started in the HRT+GnRHa group, taking after down-regulation with the GnRHa. Within the HRT group, the same dose of estradiol was commenced within the early follicular stage. The main (chemical and clinical pregnancy rates) and auxiliary results (twin pregnancy, miscarriage, and live birth rates) were compared between groups.</p><p><strong>Results: </strong>The demographic characteristics and severity of adenomyosis, endometrial thickness, and pattern at starting progesterone administration were similar in the 2 groups, and triple-line endometrium was found to be the dominant pattern in both groups (p = 0.65). No significant differences were observed in chemical, clinical, and twin pregnancy rates as well as miscarriage and live birth rates between groups (p = 0.71, p = 0.81, p = 0.11, and p = 0.84, respectively). However, the total estrogen dose and duration of estrogen consumption were significantly higher in the pretreatment group (p = 0.001, and p = 0.003).</p><p><strong>Conclusion: </strong>These results indicated that the hormonal endometrial preparation with estrogen and progestin for FET cycles is as efficacious as a protocol involving preceding pituitary suppression with a GnRHa. Further large randomized clinical studies are required to confirm these findings.</p>","PeriodicalId":14386,"journal":{"name":"International Journal of Reproductive Biomedicine","volume":"21 6","pages":"481-490"},"PeriodicalIF":1.8000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10407916/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Reproductive Biomedicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/ijrm.v21i6.13635","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Selecting a suitable and preferable method for endometrial preparation in frozen embryo transfer (FET) cycles for women with adenomyosis is still challenging in infertility treatment.
Objective: To compare 2 artificial endometrial preparation regimens with and without gonadotropin-releasing hormone agonist (GnRHa) pretreatment in women with adenomyosis undergoing FET cycles.
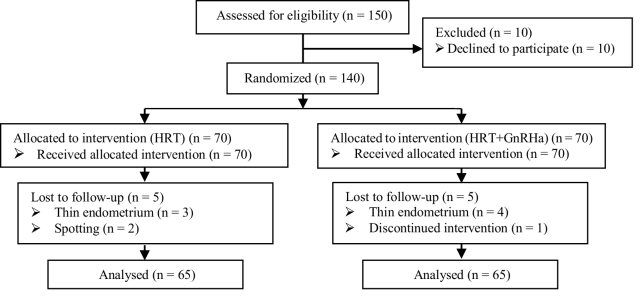
Materials and methods: This randomized clinical trial study was conducted on 140 adenomyosis cases who underwent FET cycles at Arash Women's hospital, Tehran, Iran from May 2020 to March 2021. Participants were randomly allocated into hormonal replacement therapy (HRT) and HRT+GnRHa pretreatment groups (n = 70/each). Endometrial preparation with 2-6 mg daily estradiol was started in the HRT+GnRHa group, taking after down-regulation with the GnRHa. Within the HRT group, the same dose of estradiol was commenced within the early follicular stage. The main (chemical and clinical pregnancy rates) and auxiliary results (twin pregnancy, miscarriage, and live birth rates) were compared between groups.
Results: The demographic characteristics and severity of adenomyosis, endometrial thickness, and pattern at starting progesterone administration were similar in the 2 groups, and triple-line endometrium was found to be the dominant pattern in both groups (p = 0.65). No significant differences were observed in chemical, clinical, and twin pregnancy rates as well as miscarriage and live birth rates between groups (p = 0.71, p = 0.81, p = 0.11, and p = 0.84, respectively). However, the total estrogen dose and duration of estrogen consumption were significantly higher in the pretreatment group (p = 0.001, and p = 0.003).
Conclusion: These results indicated that the hormonal endometrial preparation with estrogen and progestin for FET cycles is as efficacious as a protocol involving preceding pituitary suppression with a GnRHa. Further large randomized clinical studies are required to confirm these findings.
期刊介绍:
The International Journal of Reproductive BioMedicine (IJRM), formerly published as "Iranian Journal of Reproductive Medicine (ISSN: 1680-6433)", is an international monthly scientific journal for who treat and investigate problems of infertility and human reproductive disorders. This journal accepts Original Papers, Review Articles, Short Communications, Case Reports, Photo Clinics, and Letters to the Editor in the fields of fertility and infertility, ethical and social issues of assisted reproductive technologies, cellular and molecular biology of reproduction including the development of gametes and early embryos, assisted reproductive technologies in model system and in a clinical environment, reproductive endocrinology, andrology, epidemiology, pathology, genetics, oncology, surgery, psychology, and physiology. Emerging topics including cloning and stem cells are encouraged.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
