Eleonora Latini, Dario Buioni, Paolo Nardi, Calogera Pisano, Cristina Viscogliesi, Federico Agneni, Claudia Altieri, Giovanni Ruvolo
{"title":"Retention of temporary epicardial pacing wires: when migration causes dehiscence of a sternal wound.","authors":"Eleonora Latini, Dario Buioni, Paolo Nardi, Calogera Pisano, Cristina Viscogliesi, Federico Agneni, Claudia Altieri, Giovanni Ruvolo","doi":"10.5114/kitp.2023.129547","DOIUrl":null,"url":null,"abstract":"Address for correspondence: Dario Buioni, Cardiac Surgery Division, Tor Vergata University Hospital, Viale Oxford 81, Rome, PC 00133, Italy, e-mail: docyuk@libero.it Received: 14.02.2023, accepted: 5.03.2023. Temporary epicardial pacing wires (TEPWs) have been routinely inserted in all patients undergoing cardiac surgery since the 1960s. The main purposes were, and still are, therapeutic and diagnostic, as they are mainly used to recognize and treat ventricular and/or atrial rhythm disturbances that may be a complication of cardiac interventions and to sustain the possible hemodynamic instability during post-operative intensive care [1]. However, their necessity is often discussed as their use is linked to several but unlikely complications such as cardiac tamponade and hemorrhage at the time of removal [2], or infection, wound dehiscence and migration when retained [3]. The indications for insertion of the TEPWs are several: conduction abnormalities such as AV block, prolonged AV delay, bifascicular block; bradycardia and tachycardia, especially atrial fibrillation, which is common in the period following cardiac surgery; and the need to place both atrial and ventricular wires is often dependent on the patient; furthermore, the pacing system should be checked and reassessed routinely based on the patient’s condition. The removal must be done carefully by gentle and constant traction; if too much traction is needed as they may have been caught in a tight suture, they should be cut as close to the skin as possible due to the risk of tamponade immediately after the removal procedure. For this reason, it is necessary to observe the patient and perform echocardiography a few hours after the removal [1]. Although there is a risk of hemorrhage and cardiac tamponade, to cut the wires flush with the skin is not a procedure free of adverse events such as infection and migration. An 89-year-old woman with severe aortic stenosis and aneurysm of the ascending aorta, with medical history of hypertension, dyslipidemia, obesity and chronic renal failure, underwent aortic valve replacement with a Sorin Mitroflow 21 bioprosthesis and of the ascending aorta with an Intervascular 28 prosthesis, requiring circulatory arrest during the procedure on September 2014. In the immediate post-operative period, due to massive bleeding and hemodynamic instability, it became necessary to conduct a surgical revision of the mediastinum. Two right atrial and two right ventricular epicardial pacing wires were inserted at the moment of the intervention and were not removed during the revision of the mediastinum; on the 6th postoperative day (POD), at the time of removal, only the ones placed on the right ventricle were removed without resistance, while the ones on the right atrium were cut flush with the skin. On the 8th POD, the patient presented strong chest pain, erythema and drainage from the distal third of the sternotomy wound associated with sternal instability; on the 10th POD she became feverish and blood cultures tested positive for Proteus mirabilis and Staphylococcus epidermidis. Despite antibiotic targeted therapy there was progressive enlargement of the dehiscence and vacuum assisted closure (VAC) therapy was started. Several swabs of the wound were performed, and when they tested negative for bacterial growth, the patient underwent reconstruction of the dehiscent wound through partial mobilization of pectoralis muscles. The remaining in-hospital stay and follow-up were uneventful and the wound perfectly healed. Four years later, she came back due to the appearance of a painful swelling at the distal third of the sternotomy wound, approximately 30 mm wide; thus, empirical antibiotic therapy was started as well as serial medications of the swelling. A week after the antibiotic therapy was started, the swelling in her upper abdomen increased in volume and started to drain purulent fluid; another swab was performed and tested positive for Proteus mirabilis; therefore targeted antibiotic therapy with ciprofloxacin (500 mg/day) was started (Figure 1). The patient did not develop fever but her blood count showed the normal range of hemoglobin, 11 g/dl, increase of white blood cell count, 12,500 per μl, and C-reactive protein level of 70 g/l. As the swelling kept draining and growing despite antibiotic therapy and serial medication, the patient was hospitalized once again in January 2019 to remove the granuloma surgically. During the post-operative follow-up the wound initially presented with a superficial dehiscence that eventually reached the deep edges Retention of temporary epicardial pacing wires: when migration causes dehiscence of a sternal wound","PeriodicalId":49945,"journal":{"name":"Kardiochirurgia I Torakochirurgia Polska","volume":"20 2","pages":"123-125"},"PeriodicalIF":1.3000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ae/16/KITP-20-51120.PMC10410639.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kardiochirurgia I Torakochirurgia Polska","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/kitp.2023.129547","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
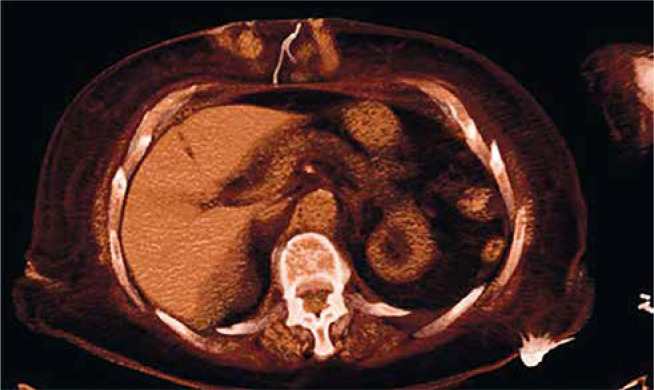
Address for correspondence: Dario Buioni, Cardiac Surgery Division, Tor Vergata University Hospital, Viale Oxford 81, Rome, PC 00133, Italy, e-mail: docyuk@libero.it Received: 14.02.2023, accepted: 5.03.2023. Temporary epicardial pacing wires (TEPWs) have been routinely inserted in all patients undergoing cardiac surgery since the 1960s. The main purposes were, and still are, therapeutic and diagnostic, as they are mainly used to recognize and treat ventricular and/or atrial rhythm disturbances that may be a complication of cardiac interventions and to sustain the possible hemodynamic instability during post-operative intensive care [1]. However, their necessity is often discussed as their use is linked to several but unlikely complications such as cardiac tamponade and hemorrhage at the time of removal [2], or infection, wound dehiscence and migration when retained [3]. The indications for insertion of the TEPWs are several: conduction abnormalities such as AV block, prolonged AV delay, bifascicular block; bradycardia and tachycardia, especially atrial fibrillation, which is common in the period following cardiac surgery; and the need to place both atrial and ventricular wires is often dependent on the patient; furthermore, the pacing system should be checked and reassessed routinely based on the patient’s condition. The removal must be done carefully by gentle and constant traction; if too much traction is needed as they may have been caught in a tight suture, they should be cut as close to the skin as possible due to the risk of tamponade immediately after the removal procedure. For this reason, it is necessary to observe the patient and perform echocardiography a few hours after the removal [1]. Although there is a risk of hemorrhage and cardiac tamponade, to cut the wires flush with the skin is not a procedure free of adverse events such as infection and migration. An 89-year-old woman with severe aortic stenosis and aneurysm of the ascending aorta, with medical history of hypertension, dyslipidemia, obesity and chronic renal failure, underwent aortic valve replacement with a Sorin Mitroflow 21 bioprosthesis and of the ascending aorta with an Intervascular 28 prosthesis, requiring circulatory arrest during the procedure on September 2014. In the immediate post-operative period, due to massive bleeding and hemodynamic instability, it became necessary to conduct a surgical revision of the mediastinum. Two right atrial and two right ventricular epicardial pacing wires were inserted at the moment of the intervention and were not removed during the revision of the mediastinum; on the 6th postoperative day (POD), at the time of removal, only the ones placed on the right ventricle were removed without resistance, while the ones on the right atrium were cut flush with the skin. On the 8th POD, the patient presented strong chest pain, erythema and drainage from the distal third of the sternotomy wound associated with sternal instability; on the 10th POD she became feverish and blood cultures tested positive for Proteus mirabilis and Staphylococcus epidermidis. Despite antibiotic targeted therapy there was progressive enlargement of the dehiscence and vacuum assisted closure (VAC) therapy was started. Several swabs of the wound were performed, and when they tested negative for bacterial growth, the patient underwent reconstruction of the dehiscent wound through partial mobilization of pectoralis muscles. The remaining in-hospital stay and follow-up were uneventful and the wound perfectly healed. Four years later, she came back due to the appearance of a painful swelling at the distal third of the sternotomy wound, approximately 30 mm wide; thus, empirical antibiotic therapy was started as well as serial medications of the swelling. A week after the antibiotic therapy was started, the swelling in her upper abdomen increased in volume and started to drain purulent fluid; another swab was performed and tested positive for Proteus mirabilis; therefore targeted antibiotic therapy with ciprofloxacin (500 mg/day) was started (Figure 1). The patient did not develop fever but her blood count showed the normal range of hemoglobin, 11 g/dl, increase of white blood cell count, 12,500 per μl, and C-reactive protein level of 70 g/l. As the swelling kept draining and growing despite antibiotic therapy and serial medication, the patient was hospitalized once again in January 2019 to remove the granuloma surgically. During the post-operative follow-up the wound initially presented with a superficial dehiscence that eventually reached the deep edges Retention of temporary epicardial pacing wires: when migration causes dehiscence of a sternal wound
期刊介绍:
Polish Journal of Thoracic and Cardiovascular Surgery is a quarterly aimed at cardiologists, cardiosurgeons and thoracic surgeons. Includes the original works (experimental, research and development), illustrative and casuistical works about cardiology and cardiosurgery.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
