J.L. Vega , A. Carrasco , N. Karim , M. Stewart , W. Bell
{"title":"一例有心血管危险因素的近SUDEP患者的复发性小脑缺血性梗死和发作期典型交感神经反应","authors":"J.L. Vega , A. Carrasco , N. Karim , M. Stewart , W. Bell","doi":"10.1016/j.ebr.2023.100605","DOIUrl":null,"url":null,"abstract":"<div><p>We report a 60-year-old woman who presented to the emergency department after experiencing a witnessed unknown onset bilateral tonic clonic seizure (GTCS) that culminated in cardiac arrest. A neurology consultant uncovered a years-long history of frequent episodic staring followed by confusion and expressive aphasia, which strongly suggested that she suffered from epilepsy. Thus, her cardiac arrest and subsequent resuscitation met criteria for a near-sudden unexpected death in epilepsy (SUDEP) diagnosis. Serial bloodwork demonstrated transient troponin I elevations and leukocytoses, while a brain MRI revealed global cerebral anoxic injury and a small acute right cerebellar ischemic infarction. A review of her medical record uncovered a hospitalization sixteen months earlier for a likely GTCS whose workup showed similar troponin I elevations and leukocytoses, and surprisingly, a different small acute right cerebellar ischemic infarction in the same vascular territory. To our knowledge, this is the first report of subcortical ischemic infarctions occurring concurrently with GTCSs in a near-SUDEP patient. Aside from illustrating the key role of inpatient neurologists in the diagnosis of near-SUDEP, this manuscript discusses the potential significance of postictal ischemic infarctions, transient asymptomatic troponin elevations, and transient non-infectious leukocytoses in epilepsy patients with cardiovascular risk factors.</p></div>","PeriodicalId":36558,"journal":{"name":"Epilepsy and Behavior Reports","volume":"23 ","pages":"Article 100605"},"PeriodicalIF":1.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10276251/pdf/","citationCount":"0","resultStr":"{\"title\":\"Recurrent cerebellar ischemic infarctions and stereotyped peri-ictal sympathetic responses in a near-SUDEP patient with cardiovascular risk factors\",\"authors\":\"J.L. Vega , A. Carrasco , N. Karim , M. Stewart , W. Bell\",\"doi\":\"10.1016/j.ebr.2023.100605\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>We report a 60-year-old woman who presented to the emergency department after experiencing a witnessed unknown onset bilateral tonic clonic seizure (GTCS) that culminated in cardiac arrest. A neurology consultant uncovered a years-long history of frequent episodic staring followed by confusion and expressive aphasia, which strongly suggested that she suffered from epilepsy. Thus, her cardiac arrest and subsequent resuscitation met criteria for a near-sudden unexpected death in epilepsy (SUDEP) diagnosis. Serial bloodwork demonstrated transient troponin I elevations and leukocytoses, while a brain MRI revealed global cerebral anoxic injury and a small acute right cerebellar ischemic infarction. A review of her medical record uncovered a hospitalization sixteen months earlier for a likely GTCS whose workup showed similar troponin I elevations and leukocytoses, and surprisingly, a different small acute right cerebellar ischemic infarction in the same vascular territory. To our knowledge, this is the first report of subcortical ischemic infarctions occurring concurrently with GTCSs in a near-SUDEP patient. Aside from illustrating the key role of inpatient neurologists in the diagnosis of near-SUDEP, this manuscript discusses the potential significance of postictal ischemic infarctions, transient asymptomatic troponin elevations, and transient non-infectious leukocytoses in epilepsy patients with cardiovascular risk factors.</p></div>\",\"PeriodicalId\":36558,\"journal\":{\"name\":\"Epilepsy and Behavior Reports\",\"volume\":\"23 \",\"pages\":\"Article 100605\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10276251/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Epilepsy and Behavior Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2589986423000230\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/5/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epilepsy and Behavior Reports","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589986423000230","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/11 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Recurrent cerebellar ischemic infarctions and stereotyped peri-ictal sympathetic responses in a near-SUDEP patient with cardiovascular risk factors
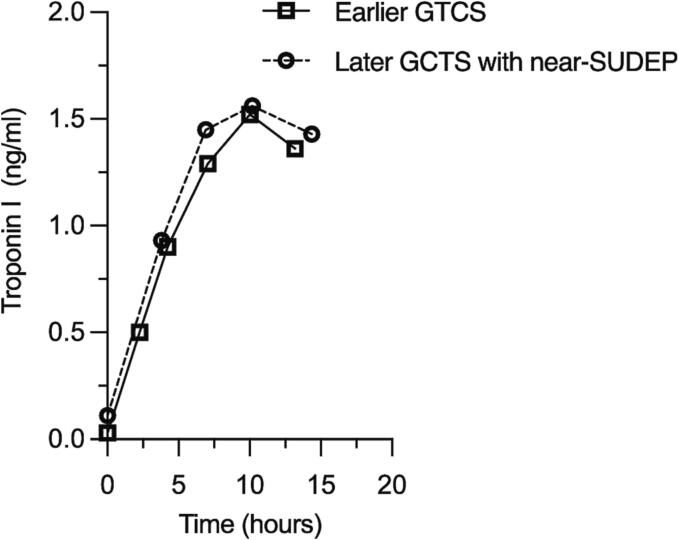
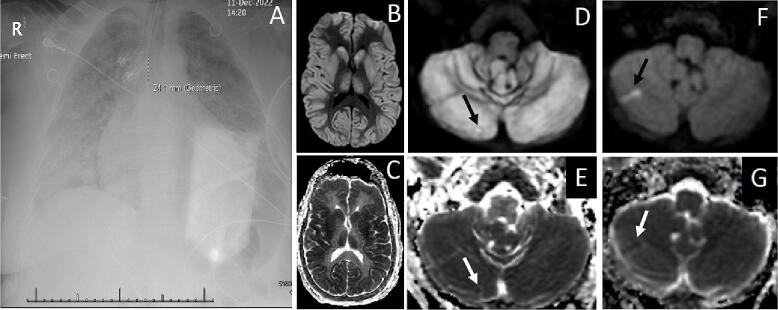
We report a 60-year-old woman who presented to the emergency department after experiencing a witnessed unknown onset bilateral tonic clonic seizure (GTCS) that culminated in cardiac arrest. A neurology consultant uncovered a years-long history of frequent episodic staring followed by confusion and expressive aphasia, which strongly suggested that she suffered from epilepsy. Thus, her cardiac arrest and subsequent resuscitation met criteria for a near-sudden unexpected death in epilepsy (SUDEP) diagnosis. Serial bloodwork demonstrated transient troponin I elevations and leukocytoses, while a brain MRI revealed global cerebral anoxic injury and a small acute right cerebellar ischemic infarction. A review of her medical record uncovered a hospitalization sixteen months earlier for a likely GTCS whose workup showed similar troponin I elevations and leukocytoses, and surprisingly, a different small acute right cerebellar ischemic infarction in the same vascular territory. To our knowledge, this is the first report of subcortical ischemic infarctions occurring concurrently with GTCSs in a near-SUDEP patient. Aside from illustrating the key role of inpatient neurologists in the diagnosis of near-SUDEP, this manuscript discusses the potential significance of postictal ischemic infarctions, transient asymptomatic troponin elevations, and transient non-infectious leukocytoses in epilepsy patients with cardiovascular risk factors.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
