{"title":"失代偿性慢性肝病和败血症儿童的低凝性:血栓弹性成像评估。","authors":"Vignesh Vinayagamoorthy, Anshu Srivastava, Indranil Das, Anupam Verma, Prabhakar Mishra, Moinak Sen Sarma, Ujjal Poddar, Surender Kumar Yachha","doi":"10.1097/PG9.0000000000000324","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the coagulation status of children with decompensated chronic liver disease (DCLD) and infection and factors affecting it using thromboelastography (TEG).</p><p><strong>Methods: </strong>Coagulation status of children admitted with DCLD and infection was assessed by international normalized ratio (INR), platelet count, and TEG [reaction time (R), kinetic time (K), α-angle (AA), maximum amplitude (MA), coagulation index (CI), and lysis index (LY30)] at admission and at 7-14 days after treatment. CI < -3 represents hypocoagulable state. Clinical profile including systemic inflammatory response syndrome (SIRS), infection severity, bleeding, treatment response, and outcome were noted.</p><p><strong>Results: </strong>Thirty children (21 boys, median (IQR) age 78 [15.7-180] months) were studied prospectively. At admission, 29 (96.7%) had prolonged INR, 24 (80%) had thrombocytopenia, and 17 (56.6%) were hypocoagulable by TEG. Nine of 30 (30%) had normal TEG but deranged INR and platelets. Nineteen (63.3%) cases had SIRS, 11 (36.6%) had severe sepsis, and 8 (26.6%) had bleeding. Hypocoagulable state was common in severe sepsis than sepsis/infection (81.1% versus 42.1%; <i>P</i> = 0.05) and persistent (n = 4) versus recovered SIRS (n = 15, 100% versus 33%; <i>P</i> = 0.03). Bleeders had prolonged R-time (7.8 versus 5.4 min; <i>P</i> = 0.03), smaller MA (30.2 versus 47 mm; <i>P</i> = 0.05), and α-angle (40.4 versus 62.9; <i>P</i> = 0.03) but similar INR and platelets than nonbleeders. Six patients (20%) had poor in-hospital outcomes; R-time ≥8.5 min predicted mortality with high sensitivity (83%) and specificity (100%).</p><p><strong>Conclusions: </strong>Fifth-seven percent of children with DCLD and infection were hypocoagulable by TEG. Severe sepsis and persistent SIRS worsened the coagulation status. TEG identifies bleeders better than INR and platelet count. R-time ≥8.5 min predicts a poor hospital outcome.</p>","PeriodicalId":17618,"journal":{"name":"JPGN Reports","volume":"4 3","pages":"e324"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10435032/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hypocoagulability in Children With Decompensated Chronic Liver Disease and Sepsis: Assessment by Thromboelastography.\",\"authors\":\"Vignesh Vinayagamoorthy, Anshu Srivastava, Indranil Das, Anupam Verma, Prabhakar Mishra, Moinak Sen Sarma, Ujjal Poddar, Surender Kumar Yachha\",\"doi\":\"10.1097/PG9.0000000000000324\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To evaluate the coagulation status of children with decompensated chronic liver disease (DCLD) and infection and factors affecting it using thromboelastography (TEG).</p><p><strong>Methods: </strong>Coagulation status of children admitted with DCLD and infection was assessed by international normalized ratio (INR), platelet count, and TEG [reaction time (R), kinetic time (K), α-angle (AA), maximum amplitude (MA), coagulation index (CI), and lysis index (LY30)] at admission and at 7-14 days after treatment. CI < -3 represents hypocoagulable state. Clinical profile including systemic inflammatory response syndrome (SIRS), infection severity, bleeding, treatment response, and outcome were noted.</p><p><strong>Results: </strong>Thirty children (21 boys, median (IQR) age 78 [15.7-180] months) were studied prospectively. At admission, 29 (96.7%) had prolonged INR, 24 (80%) had thrombocytopenia, and 17 (56.6%) were hypocoagulable by TEG. Nine of 30 (30%) had normal TEG but deranged INR and platelets. Nineteen (63.3%) cases had SIRS, 11 (36.6%) had severe sepsis, and 8 (26.6%) had bleeding. Hypocoagulable state was common in severe sepsis than sepsis/infection (81.1% versus 42.1%; <i>P</i> = 0.05) and persistent (n = 4) versus recovered SIRS (n = 15, 100% versus 33%; <i>P</i> = 0.03). Bleeders had prolonged R-time (7.8 versus 5.4 min; <i>P</i> = 0.03), smaller MA (30.2 versus 47 mm; <i>P</i> = 0.05), and α-angle (40.4 versus 62.9; <i>P</i> = 0.03) but similar INR and platelets than nonbleeders. Six patients (20%) had poor in-hospital outcomes; R-time ≥8.5 min predicted mortality with high sensitivity (83%) and specificity (100%).</p><p><strong>Conclusions: </strong>Fifth-seven percent of children with DCLD and infection were hypocoagulable by TEG. Severe sepsis and persistent SIRS worsened the coagulation status. TEG identifies bleeders better than INR and platelet count. R-time ≥8.5 min predicts a poor hospital outcome.</p>\",\"PeriodicalId\":17618,\"journal\":{\"name\":\"JPGN Reports\",\"volume\":\"4 3\",\"pages\":\"e324\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10435032/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JPGN Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/PG9.0000000000000324\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JPGN Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/PG9.0000000000000324","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Hypocoagulability in Children With Decompensated Chronic Liver Disease and Sepsis: Assessment by Thromboelastography.
Objective: To evaluate the coagulation status of children with decompensated chronic liver disease (DCLD) and infection and factors affecting it using thromboelastography (TEG).
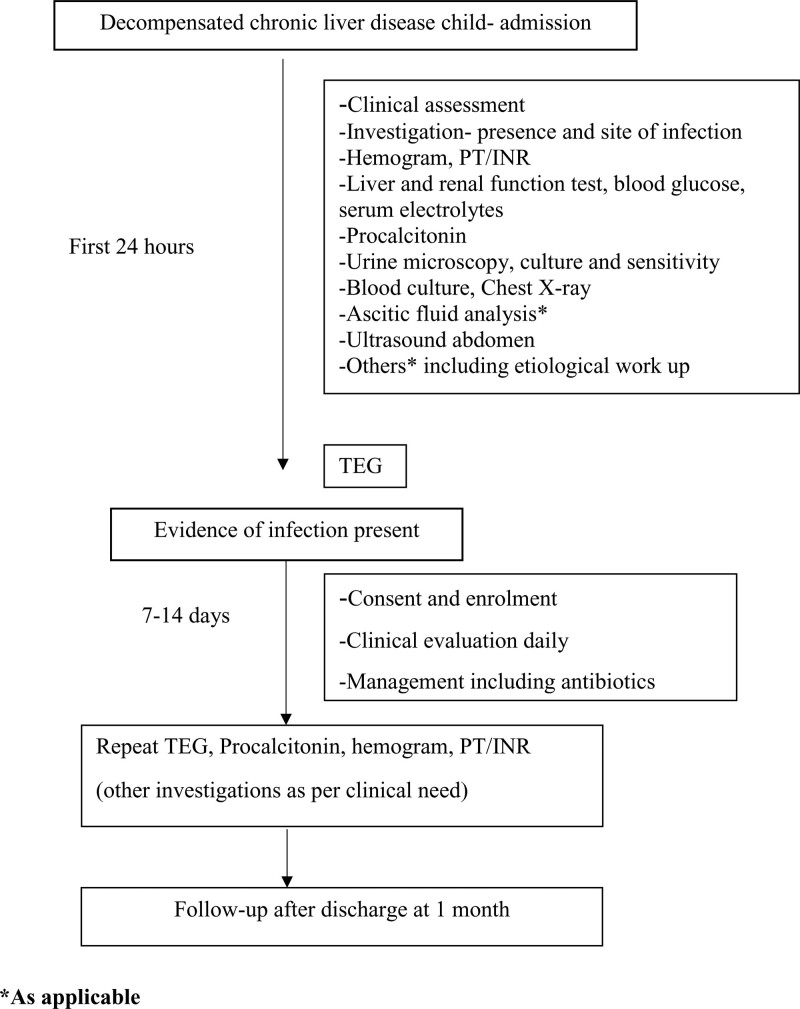
Methods: Coagulation status of children admitted with DCLD and infection was assessed by international normalized ratio (INR), platelet count, and TEG [reaction time (R), kinetic time (K), α-angle (AA), maximum amplitude (MA), coagulation index (CI), and lysis index (LY30)] at admission and at 7-14 days after treatment. CI < -3 represents hypocoagulable state. Clinical profile including systemic inflammatory response syndrome (SIRS), infection severity, bleeding, treatment response, and outcome were noted.
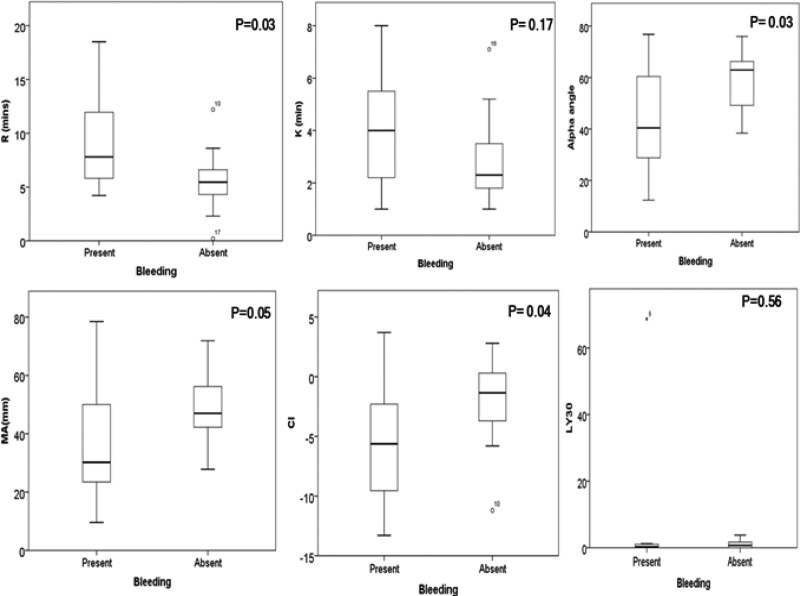
Results: Thirty children (21 boys, median (IQR) age 78 [15.7-180] months) were studied prospectively. At admission, 29 (96.7%) had prolonged INR, 24 (80%) had thrombocytopenia, and 17 (56.6%) were hypocoagulable by TEG. Nine of 30 (30%) had normal TEG but deranged INR and platelets. Nineteen (63.3%) cases had SIRS, 11 (36.6%) had severe sepsis, and 8 (26.6%) had bleeding. Hypocoagulable state was common in severe sepsis than sepsis/infection (81.1% versus 42.1%; P = 0.05) and persistent (n = 4) versus recovered SIRS (n = 15, 100% versus 33%; P = 0.03). Bleeders had prolonged R-time (7.8 versus 5.4 min; P = 0.03), smaller MA (30.2 versus 47 mm; P = 0.05), and α-angle (40.4 versus 62.9; P = 0.03) but similar INR and platelets than nonbleeders. Six patients (20%) had poor in-hospital outcomes; R-time ≥8.5 min predicted mortality with high sensitivity (83%) and specificity (100%).
Conclusions: Fifth-seven percent of children with DCLD and infection were hypocoagulable by TEG. Severe sepsis and persistent SIRS worsened the coagulation status. TEG identifies bleeders better than INR and platelet count. R-time ≥8.5 min predicts a poor hospital outcome.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
