Amber Meservey, Govind Krishnan, Cynthia L Green, Samantha Morrison, Craig R Rackley, Bryan D Kraft
{"title":"接受静脉体外膜氧合的急性呼吸窘迫综合征患者体内羧基血红蛋白与死亡率之间的 U 型关系","authors":"Amber Meservey, Govind Krishnan, Cynthia L Green, Samantha Morrison, Craig R Rackley, Bryan D Kraft","doi":"10.1097/CCE.0000000000000957","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Carbon monoxide (CO) is an endogenous signaling molecule that activates cytoprotective programs implicated in the resolution of acute respiratory distress syndrome (ARDS) and survival of critical illness. Because CO levels can be measured in blood as carboxyhemoglobin, we hypothesized that carboxyhemoglobin percent (COHb%) may associate with mortality.</p><p><strong>Objectives: </strong>To examine the relationship between COHb% and outcomes in patients with ARDS requiring venovenous extracorporeal membrane oxygenation (ECMO), a condition where elevated COHb% is commonly observed.</p><p><strong>Design: </strong>Retrospective cohort study.</p><p><strong>Setting: </strong>Academic medical center ICU.</p><p><strong>Patients: </strong>Patients were included that had ARDS on venovenous ECMO.</p><p><strong>Measurements and main results: </strong>We examined the association between COHb% and mortality using a Cox proportional hazards model. Secondary outcomes including ECMO duration, ventilator weaning, and hospital and ICU length of stay were examined using both subdistribution and causal-specific hazard models for competing risks. We identified 109 consecutive patients for analysis. Mortality significantly decreased per 1 U increase in COHb% below 3.25% (hazard ratio [HR], 0.35; 95% CI, 0.15-0.80; <i>p</i> = 0.013) and increased per 1 U increase above 3.25% (HR, 4.7; 95% CI, 1.5-14.7; <i>p</i> = 0.007) reflecting a nonlinear association (<i>p</i> = 0.006). Each unit increase in COHb% was associated with reduced likelihood of liberation from ECMO and mechanical ventilation, and increased time to hospital and ICU discharge (all <i>p</i> < 0.05). COHb% was significantly associated with hemolysis but not with initiation of hemodialysis or blood transfusions.</p><p><strong>Conclusions: </strong>In patients with ARDS on venovenous ECMO, COHb% is a novel biomarker for mortality exhibiting a U-shaped pattern. Our findings suggest that too little CO (perhaps due to impaired host signaling) or excess CO (perhaps due to hemolysis) is associated with higher mortality. Patients with low COHb% may exhibit the most benefit from future therapies targeting anti-oxidant and anti-inflammatory pathways such as low-dose inhaled CO gas.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 8","pages":"e0957"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c4/19/cc9-5-e0957.PMC10443764.pdf","citationCount":"0","resultStr":"{\"title\":\"U-Shaped Association Between Carboxyhemoglobin and Mortality in Patients With Acute Respiratory Distress Syndrome on Venovenous Extracorporeal Membrane Oxygenation.\",\"authors\":\"Amber Meservey, Govind Krishnan, Cynthia L Green, Samantha Morrison, Craig R Rackley, Bryan D Kraft\",\"doi\":\"10.1097/CCE.0000000000000957\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Carbon monoxide (CO) is an endogenous signaling molecule that activates cytoprotective programs implicated in the resolution of acute respiratory distress syndrome (ARDS) and survival of critical illness. Because CO levels can be measured in blood as carboxyhemoglobin, we hypothesized that carboxyhemoglobin percent (COHb%) may associate with mortality.</p><p><strong>Objectives: </strong>To examine the relationship between COHb% and outcomes in patients with ARDS requiring venovenous extracorporeal membrane oxygenation (ECMO), a condition where elevated COHb% is commonly observed.</p><p><strong>Design: </strong>Retrospective cohort study.</p><p><strong>Setting: </strong>Academic medical center ICU.</p><p><strong>Patients: </strong>Patients were included that had ARDS on venovenous ECMO.</p><p><strong>Measurements and main results: </strong>We examined the association between COHb% and mortality using a Cox proportional hazards model. Secondary outcomes including ECMO duration, ventilator weaning, and hospital and ICU length of stay were examined using both subdistribution and causal-specific hazard models for competing risks. We identified 109 consecutive patients for analysis. Mortality significantly decreased per 1 U increase in COHb% below 3.25% (hazard ratio [HR], 0.35; 95% CI, 0.15-0.80; <i>p</i> = 0.013) and increased per 1 U increase above 3.25% (HR, 4.7; 95% CI, 1.5-14.7; <i>p</i> = 0.007) reflecting a nonlinear association (<i>p</i> = 0.006). Each unit increase in COHb% was associated with reduced likelihood of liberation from ECMO and mechanical ventilation, and increased time to hospital and ICU discharge (all <i>p</i> < 0.05). COHb% was significantly associated with hemolysis but not with initiation of hemodialysis or blood transfusions.</p><p><strong>Conclusions: </strong>In patients with ARDS on venovenous ECMO, COHb% is a novel biomarker for mortality exhibiting a U-shaped pattern. Our findings suggest that too little CO (perhaps due to impaired host signaling) or excess CO (perhaps due to hemolysis) is associated with higher mortality. Patients with low COHb% may exhibit the most benefit from future therapies targeting anti-oxidant and anti-inflammatory pathways such as low-dose inhaled CO gas.</p>\",\"PeriodicalId\":10759,\"journal\":{\"name\":\"Critical Care Explorations\",\"volume\":\"5 8\",\"pages\":\"e0957\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c4/19/cc9-5-e0957.PMC10443764.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000000957\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000957","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:一氧化碳(CO)是一种激活细胞保护程序的内源性信号分子,与急性呼吸窘迫综合征(ARDS)的缓解和危重病人的存活有关。由于 CO 水平可在血液中以碳氧血红蛋白的形式测量,我们假设碳氧血红蛋白百分比(COHb%)可能与死亡率有关:研究需要静脉体外膜氧合(ECMO)的 ARDS 患者 COHb% 与预后之间的关系:设计:回顾性队列研究:背景:学术医疗中心重症监护室:研究对象:使用静脉 ECMO 的 ARDS 患者:我们使用 Cox 比例危险模型研究了 COHb% 与死亡率之间的关系。次要结果包括 ECMO 持续时间、呼吸机断流、住院时间和重症监护室停留时间,我们使用了子分布和因果特异性危险模型来研究竞争风险。我们确定了 109 名连续患者进行分析。COHb% 低于 3.25% 时,死亡率每增加 1 U 就会明显下降(危险比 [HR],0.35;95% CI,0.15-0.80;p = 0.013),而高于 3.25% 时,死亡率每增加 1 U 就会上升(HR,4.7;95% CI,1.5-14.7;p = 0.007),这反映了一种非线性关联(p = 0.006)。COHb% 每增加一个单位,就会降低脱离 ECMO 和机械通气的可能性,并延长住院时间和 ICU 出院时间(所有 p <0.05)。COHb% 与溶血显著相关,但与开始血液透析或输血无关:结论:在使用静脉 ECMO 的 ARDS 患者中,COHb% 是一种新的死亡率生物标志物,呈现 U 型模式。我们的研究结果表明,过低的 CO(可能是由于宿主信号受损)或过高的 CO(可能是由于溶血)与较高的死亡率相关。COHb% 低的患者可能从未来针对抗氧化和抗炎途径的疗法(如低剂量吸入 CO 气体)中获益最多。
U-Shaped Association Between Carboxyhemoglobin and Mortality in Patients With Acute Respiratory Distress Syndrome on Venovenous Extracorporeal Membrane Oxygenation.
Background: Carbon monoxide (CO) is an endogenous signaling molecule that activates cytoprotective programs implicated in the resolution of acute respiratory distress syndrome (ARDS) and survival of critical illness. Because CO levels can be measured in blood as carboxyhemoglobin, we hypothesized that carboxyhemoglobin percent (COHb%) may associate with mortality.
Objectives: To examine the relationship between COHb% and outcomes in patients with ARDS requiring venovenous extracorporeal membrane oxygenation (ECMO), a condition where elevated COHb% is commonly observed.
Design: Retrospective cohort study.
Setting: Academic medical center ICU.
Patients: Patients were included that had ARDS on venovenous ECMO.
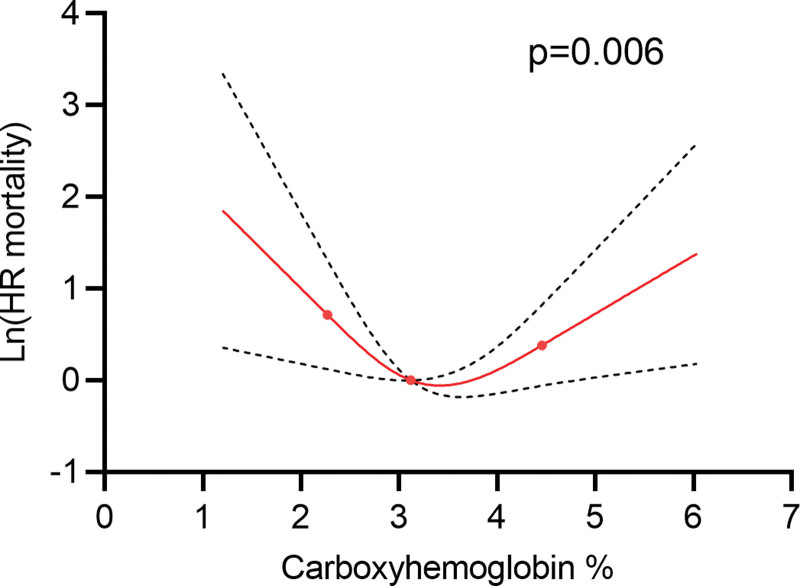
Measurements and main results: We examined the association between COHb% and mortality using a Cox proportional hazards model. Secondary outcomes including ECMO duration, ventilator weaning, and hospital and ICU length of stay were examined using both subdistribution and causal-specific hazard models for competing risks. We identified 109 consecutive patients for analysis. Mortality significantly decreased per 1 U increase in COHb% below 3.25% (hazard ratio [HR], 0.35; 95% CI, 0.15-0.80; p = 0.013) and increased per 1 U increase above 3.25% (HR, 4.7; 95% CI, 1.5-14.7; p = 0.007) reflecting a nonlinear association (p = 0.006). Each unit increase in COHb% was associated with reduced likelihood of liberation from ECMO and mechanical ventilation, and increased time to hospital and ICU discharge (all p < 0.05). COHb% was significantly associated with hemolysis but not with initiation of hemodialysis or blood transfusions.
Conclusions: In patients with ARDS on venovenous ECMO, COHb% is a novel biomarker for mortality exhibiting a U-shaped pattern. Our findings suggest that too little CO (perhaps due to impaired host signaling) or excess CO (perhaps due to hemolysis) is associated with higher mortality. Patients with low COHb% may exhibit the most benefit from future therapies targeting anti-oxidant and anti-inflammatory pathways such as low-dose inhaled CO gas.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
