{"title":"Acalabrutinib和类固醇治疗复发性慢性淋巴细胞白血病伴严重骨髓浸润引起的自身免疫性血小板减少症。","authors":"Takashi Oyama, Megumi Yasunaga, Masahiro Jona, Masako Nishikawa, Yutaka Yatomi, Akira Honda, Hiroaki Maki, Ken Morita, Yosuke Masamoto, Mineo Kurokawa","doi":"10.3960/jslrt.23023","DOIUrl":null,"url":null,"abstract":"<p><p>Thrombocytopenia is a frequent complication in chronic lymphocytic leukemia (CLL). Differentiating autoimmune thrombocytopenia from thrombocytopenia due to bone marrow infiltration is necessary for appropriate treatment, but sometimes difficult. Here we report a 60-year-old male patient with CLL who had achieved complete response after treatment with fludarabine, cyclophosphamide, and rituximab two years prior to presentation. He was admitted with severe thrombocytopenia that was unresponsive to intravenous immunoglobulin. Imaging studies revealed systemic enlarged lymph nodes and bone marrow aspiration was hypercellular with > 95% lymphocytes and scant megakaryocytes. Acalabrutinib 200 mg/day was administered for the treatment of CLL exacerbation. A gradual decrease in CLL cells and recovery of megakaryocytes in bone marrow were observed, but platelet counts remained low. Systemic administration of prednisolone 0.5 mg/kg, in addition to acalabrutinib, was started, considering the contribution of autoimmune thrombocytopenia; platelet recovery was rapid and sustained for more than a year. Even if bone marrow examination suggested thrombocytopenia due to direct leukemic infiltration, it is difficult to exclude the possibility of concomitant immunogenic thrombocytopenia. We conclude that for CLL patients with severe thrombocytopenia, repeating bone marrow examination and concurrent immunosuppressive therapies and treatment of the underlying CLL may be beneficial.</p>","PeriodicalId":45936,"journal":{"name":"Journal of Clinical and Experimental Hematopathology","volume":" ","pages":"187-192"},"PeriodicalIF":1.4000,"publicationDate":"2023-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10628828/pdf/","citationCount":"0","resultStr":"{\"title\":\"Acalabrutinib and steroid for autoimmune thrombocytopenia due to relapsed chronic lymphocytic leukemia with severe bone marrow infiltration.\",\"authors\":\"Takashi Oyama, Megumi Yasunaga, Masahiro Jona, Masako Nishikawa, Yutaka Yatomi, Akira Honda, Hiroaki Maki, Ken Morita, Yosuke Masamoto, Mineo Kurokawa\",\"doi\":\"10.3960/jslrt.23023\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Thrombocytopenia is a frequent complication in chronic lymphocytic leukemia (CLL). Differentiating autoimmune thrombocytopenia from thrombocytopenia due to bone marrow infiltration is necessary for appropriate treatment, but sometimes difficult. Here we report a 60-year-old male patient with CLL who had achieved complete response after treatment with fludarabine, cyclophosphamide, and rituximab two years prior to presentation. He was admitted with severe thrombocytopenia that was unresponsive to intravenous immunoglobulin. Imaging studies revealed systemic enlarged lymph nodes and bone marrow aspiration was hypercellular with > 95% lymphocytes and scant megakaryocytes. Acalabrutinib 200 mg/day was administered for the treatment of CLL exacerbation. A gradual decrease in CLL cells and recovery of megakaryocytes in bone marrow were observed, but platelet counts remained low. Systemic administration of prednisolone 0.5 mg/kg, in addition to acalabrutinib, was started, considering the contribution of autoimmune thrombocytopenia; platelet recovery was rapid and sustained for more than a year. Even if bone marrow examination suggested thrombocytopenia due to direct leukemic infiltration, it is difficult to exclude the possibility of concomitant immunogenic thrombocytopenia. We conclude that for CLL patients with severe thrombocytopenia, repeating bone marrow examination and concurrent immunosuppressive therapies and treatment of the underlying CLL may be beneficial.</p>\",\"PeriodicalId\":45936,\"journal\":{\"name\":\"Journal of Clinical and Experimental Hematopathology\",\"volume\":\" \",\"pages\":\"187-192\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-09-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10628828/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical and Experimental Hematopathology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3960/jslrt.23023\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Experimental Hematopathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3960/jslrt.23023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/28 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Acalabrutinib and steroid for autoimmune thrombocytopenia due to relapsed chronic lymphocytic leukemia with severe bone marrow infiltration.
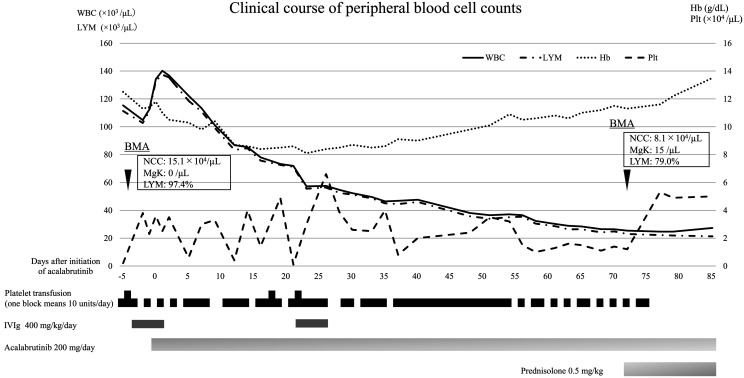
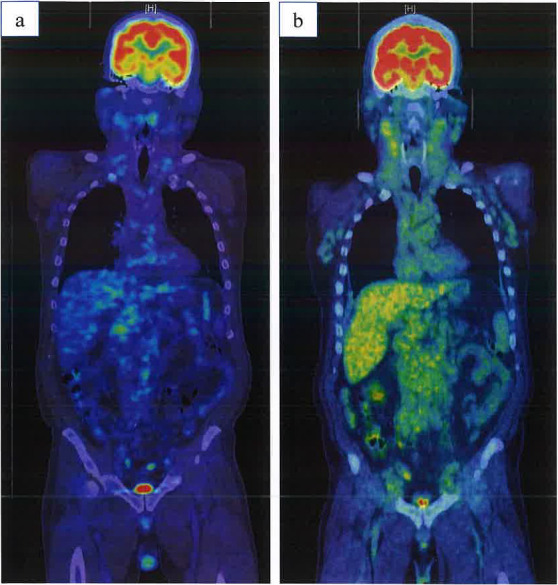
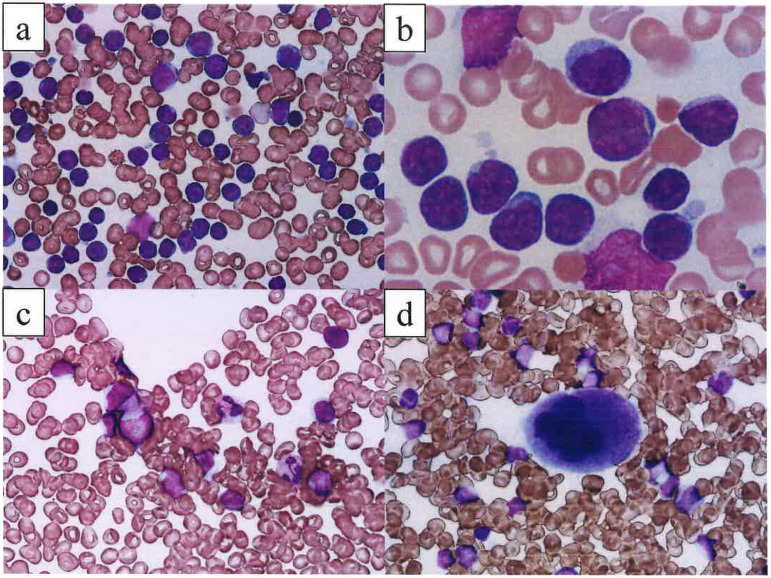
Thrombocytopenia is a frequent complication in chronic lymphocytic leukemia (CLL). Differentiating autoimmune thrombocytopenia from thrombocytopenia due to bone marrow infiltration is necessary for appropriate treatment, but sometimes difficult. Here we report a 60-year-old male patient with CLL who had achieved complete response after treatment with fludarabine, cyclophosphamide, and rituximab two years prior to presentation. He was admitted with severe thrombocytopenia that was unresponsive to intravenous immunoglobulin. Imaging studies revealed systemic enlarged lymph nodes and bone marrow aspiration was hypercellular with > 95% lymphocytes and scant megakaryocytes. Acalabrutinib 200 mg/day was administered for the treatment of CLL exacerbation. A gradual decrease in CLL cells and recovery of megakaryocytes in bone marrow were observed, but platelet counts remained low. Systemic administration of prednisolone 0.5 mg/kg, in addition to acalabrutinib, was started, considering the contribution of autoimmune thrombocytopenia; platelet recovery was rapid and sustained for more than a year. Even if bone marrow examination suggested thrombocytopenia due to direct leukemic infiltration, it is difficult to exclude the possibility of concomitant immunogenic thrombocytopenia. We conclude that for CLL patients with severe thrombocytopenia, repeating bone marrow examination and concurrent immunosuppressive therapies and treatment of the underlying CLL may be beneficial.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
