Michael S Kelly, Adna Mohammed, Daniel Okin, George A Alba, Sirus J Jesudasen, Shelby Flanagan, Nupur A Dandawate, Alexander Gavralidis, Leslie L Chang, Emily E Moin, Alison S Witkin, Kathryn A Hibbert, Aran Kadar, Patrick L Gordan, Lisa M Bebell, Marissa Hauptman, Linda Valeri, Peggy S Lai
{"title":"首选语言介导COVID-19危重患者的种族、民族和延迟表现之间的关联","authors":"Michael S Kelly, Adna Mohammed, Daniel Okin, George A Alba, Sirus J Jesudasen, Shelby Flanagan, Nupur A Dandawate, Alexander Gavralidis, Leslie L Chang, Emily E Moin, Alison S Witkin, Kathryn A Hibbert, Aran Kadar, Patrick L Gordan, Lisa M Bebell, Marissa Hauptman, Linda Valeri, Peggy S Lai","doi":"10.1097/CCE.0000000000000927","DOIUrl":null,"url":null,"abstract":"<p><p>Which social factors explain racial and ethnic disparities in COVID-19 access to care and outcomes remain unclear.</p><p><strong>Objectives: </strong>We hypothesized that preferred language mediates the association between race, ethnicity and delays to care.</p><p><strong>Design setting and participants: </strong>Multicenter, retrospective cohort study of adults with COVID-19 consecutively admitted to the ICU in three Massachusetts hospitals in 2020.</p><p><strong>Main outcome and measures: </strong>Causal mediation analysis was performed to evaluate potential mediators including preferred language, insurance status, and neighborhood characteristics.</p><p><strong>Results: </strong>Non-Hispanic White (NHW) patients (157/442, 36%) were more likely to speak English as their preferred language (78% vs. 13%), were less likely to be un- or under-insured (1% vs. 28%), lived in neighborhoods with lower social vulnerability index (SVI) than patients from racial and ethnic minority groups (SVI percentile 59 [28] vs. 74 [21]) but had more comorbidities (Charlson comorbidity index 4.6 [2.5] vs. 3.0 [2.5]), and were older (70 [13.2] vs. 58 [15.1] years). From symptom onset, NHW patients were admitted 1.67 [0.71-2.63] days earlier than patients from racial and ethnic minority groups (<i>p</i> < 0.01). Non-English preferred language was associated with delay to admission of 1.29 [0.40-2.18] days (<i>p</i> < 0.01). Preferred language mediated 63% of the total effect (<i>p</i> = 0.02) between race, ethnicity and days from symptom onset to hospital admission. Insurance status, social vulnerability, and distance to the hospital were not on the causal pathway between race, ethnicity and delay to admission.</p><p><strong>Conclusions and relevance: </strong>Preferred language mediates the association between race, ethnicity and delays to presentation for critically ill patients with COVID-19, although our results are limited by possible collider stratification bias. Effective COVID-19 treatments require early diagnosis, and delays are associated with increased mortality. Further research on the role preferred language plays in racial and ethnic disparities may identify effective solutions for equitable care.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 6","pages":"e0927"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/14/32/cc9-5-e0927.PMC10270487.pdf","citationCount":"0","resultStr":"{\"title\":\"Preferred Language Mediates Association Between Race, Ethnicity, and Delayed Presentation in Critically Ill Patients With COVID-19.\",\"authors\":\"Michael S Kelly, Adna Mohammed, Daniel Okin, George A Alba, Sirus J Jesudasen, Shelby Flanagan, Nupur A Dandawate, Alexander Gavralidis, Leslie L Chang, Emily E Moin, Alison S Witkin, Kathryn A Hibbert, Aran Kadar, Patrick L Gordan, Lisa M Bebell, Marissa Hauptman, Linda Valeri, Peggy S Lai\",\"doi\":\"10.1097/CCE.0000000000000927\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Which social factors explain racial and ethnic disparities in COVID-19 access to care and outcomes remain unclear.</p><p><strong>Objectives: </strong>We hypothesized that preferred language mediates the association between race, ethnicity and delays to care.</p><p><strong>Design setting and participants: </strong>Multicenter, retrospective cohort study of adults with COVID-19 consecutively admitted to the ICU in three Massachusetts hospitals in 2020.</p><p><strong>Main outcome and measures: </strong>Causal mediation analysis was performed to evaluate potential mediators including preferred language, insurance status, and neighborhood characteristics.</p><p><strong>Results: </strong>Non-Hispanic White (NHW) patients (157/442, 36%) were more likely to speak English as their preferred language (78% vs. 13%), were less likely to be un- or under-insured (1% vs. 28%), lived in neighborhoods with lower social vulnerability index (SVI) than patients from racial and ethnic minority groups (SVI percentile 59 [28] vs. 74 [21]) but had more comorbidities (Charlson comorbidity index 4.6 [2.5] vs. 3.0 [2.5]), and were older (70 [13.2] vs. 58 [15.1] years). From symptom onset, NHW patients were admitted 1.67 [0.71-2.63] days earlier than patients from racial and ethnic minority groups (<i>p</i> < 0.01). Non-English preferred language was associated with delay to admission of 1.29 [0.40-2.18] days (<i>p</i> < 0.01). Preferred language mediated 63% of the total effect (<i>p</i> = 0.02) between race, ethnicity and days from symptom onset to hospital admission. Insurance status, social vulnerability, and distance to the hospital were not on the causal pathway between race, ethnicity and delay to admission.</p><p><strong>Conclusions and relevance: </strong>Preferred language mediates the association between race, ethnicity and delays to presentation for critically ill patients with COVID-19, although our results are limited by possible collider stratification bias. Effective COVID-19 treatments require early diagnosis, and delays are associated with increased mortality. Further research on the role preferred language plays in racial and ethnic disparities may identify effective solutions for equitable care.</p>\",\"PeriodicalId\":10759,\"journal\":{\"name\":\"Critical Care Explorations\",\"volume\":\"5 6\",\"pages\":\"e0927\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/14/32/cc9-5-e0927.PMC10270487.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000000927\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000927","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Preferred Language Mediates Association Between Race, Ethnicity, and Delayed Presentation in Critically Ill Patients With COVID-19.
Which social factors explain racial and ethnic disparities in COVID-19 access to care and outcomes remain unclear.
Objectives: We hypothesized that preferred language mediates the association between race, ethnicity and delays to care.
Design setting and participants: Multicenter, retrospective cohort study of adults with COVID-19 consecutively admitted to the ICU in three Massachusetts hospitals in 2020.
Main outcome and measures: Causal mediation analysis was performed to evaluate potential mediators including preferred language, insurance status, and neighborhood characteristics.
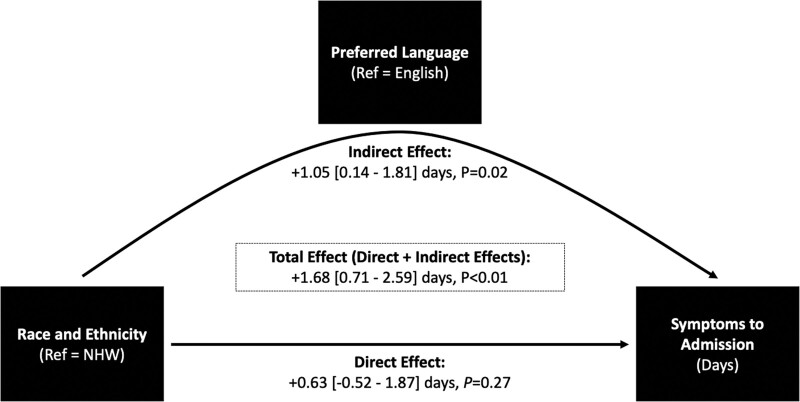
Results: Non-Hispanic White (NHW) patients (157/442, 36%) were more likely to speak English as their preferred language (78% vs. 13%), were less likely to be un- or under-insured (1% vs. 28%), lived in neighborhoods with lower social vulnerability index (SVI) than patients from racial and ethnic minority groups (SVI percentile 59 [28] vs. 74 [21]) but had more comorbidities (Charlson comorbidity index 4.6 [2.5] vs. 3.0 [2.5]), and were older (70 [13.2] vs. 58 [15.1] years). From symptom onset, NHW patients were admitted 1.67 [0.71-2.63] days earlier than patients from racial and ethnic minority groups (p < 0.01). Non-English preferred language was associated with delay to admission of 1.29 [0.40-2.18] days (p < 0.01). Preferred language mediated 63% of the total effect (p = 0.02) between race, ethnicity and days from symptom onset to hospital admission. Insurance status, social vulnerability, and distance to the hospital were not on the causal pathway between race, ethnicity and delay to admission.
Conclusions and relevance: Preferred language mediates the association between race, ethnicity and delays to presentation for critically ill patients with COVID-19, although our results are limited by possible collider stratification bias. Effective COVID-19 treatments require early diagnosis, and delays are associated with increased mortality. Further research on the role preferred language plays in racial and ethnic disparities may identify effective solutions for equitable care.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
