Luís Fabião, Ana Ribau, Carolina Lemos, Ricardo Rodrigues-Pinto
{"title":"术中透视放射在骨科创伤中的应用:与手术类型和外科医生经验的关系。","authors":"Luís Fabião, Ana Ribau, Carolina Lemos, Ricardo Rodrigues-Pinto","doi":"10.1097/j.pbj.0000000000000218","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While fluoroscopy is widely used in orthopedic trauma surgeries, it is associated with harmful effects and should, therefore, be minimized. However, reference values for these surgeries have not been defined, and it is not known how surgeon experience affects these factors. The aims of this study were to analyze the radiation emitted and exposure time for common orthopedic trauma surgeries and to assess whether they are affected by surgeon experience.</p><p><strong>Methods: </strong>Data from 1842 trauma orthopedic procedures were retrospectively analyzed. A total of 1421 procedures were included in the analysis. Radiation dose and time were collected to identify reference values for each surgery and compared for when the lead surgeon was a young resident, a senior resident, or a specialist.</p><p><strong>Results: </strong>The most performed surgeries requiring fluoroscopy were proximal femur short intramedullary nailing (n = 401), ankle open reduction and internal fixation (ORIF) (n = 141), distal radius ORIF (n = 125), and proximal femur dynamic hip screw (DHS) (n = 114). Surgeries using higher radiation dose were proximal femur long intramedullary nailing (mean dose area [DAP]): 1361.35 mGycm<sup>2</sup>), proximal femur DHS (1094.81 mGycm<sup>2</sup>), and proximal femur short intramedullary nailing (891.41 mGycm<sup>2</sup>). Surgeries requiring longer radiation time were proximal humerus and/or humeral shaft intramedullary nailing (02 mm:20 ss), proximal femur long intramedullary nailing (02 mm:04 ss), and tibial shaft/distal tibia intramedullary nailing (01 mm:49 ss). Senior residents required shorter radiation time when performing short intramedullary nailing of the proximal femur than young residents. Specialists required more radiation dose than residents when performing tibial nailing and tibial plateau ORIF and required longer radiation time than young residents when performing tibial nailing.</p><p><strong>Conclusions: </strong>This study presents mean values of radiation dose and time for common orthopedic trauma surgeries. Orthopedic surgeon experience influences radiation dose and time values. Contrary to expected, less experience is associated with lower values in some of the cases analyzed.</p>","PeriodicalId":74479,"journal":{"name":"Porto biomedical journal","volume":"8 3","pages":"e218"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0e/26/pj9-8-e218.PMC10289723.pdf","citationCount":"1","resultStr":"{\"title\":\"Intraoperative fluoroscopic radiation in orthopedic trauma: correlation with surgery type and surgeon experience.\",\"authors\":\"Luís Fabião, Ana Ribau, Carolina Lemos, Ricardo Rodrigues-Pinto\",\"doi\":\"10.1097/j.pbj.0000000000000218\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>While fluoroscopy is widely used in orthopedic trauma surgeries, it is associated with harmful effects and should, therefore, be minimized. However, reference values for these surgeries have not been defined, and it is not known how surgeon experience affects these factors. The aims of this study were to analyze the radiation emitted and exposure time for common orthopedic trauma surgeries and to assess whether they are affected by surgeon experience.</p><p><strong>Methods: </strong>Data from 1842 trauma orthopedic procedures were retrospectively analyzed. A total of 1421 procedures were included in the analysis. Radiation dose and time were collected to identify reference values for each surgery and compared for when the lead surgeon was a young resident, a senior resident, or a specialist.</p><p><strong>Results: </strong>The most performed surgeries requiring fluoroscopy were proximal femur short intramedullary nailing (n = 401), ankle open reduction and internal fixation (ORIF) (n = 141), distal radius ORIF (n = 125), and proximal femur dynamic hip screw (DHS) (n = 114). Surgeries using higher radiation dose were proximal femur long intramedullary nailing (mean dose area [DAP]): 1361.35 mGycm<sup>2</sup>), proximal femur DHS (1094.81 mGycm<sup>2</sup>), and proximal femur short intramedullary nailing (891.41 mGycm<sup>2</sup>). Surgeries requiring longer radiation time were proximal humerus and/or humeral shaft intramedullary nailing (02 mm:20 ss), proximal femur long intramedullary nailing (02 mm:04 ss), and tibial shaft/distal tibia intramedullary nailing (01 mm:49 ss). Senior residents required shorter radiation time when performing short intramedullary nailing of the proximal femur than young residents. Specialists required more radiation dose than residents when performing tibial nailing and tibial plateau ORIF and required longer radiation time than young residents when performing tibial nailing.</p><p><strong>Conclusions: </strong>This study presents mean values of radiation dose and time for common orthopedic trauma surgeries. Orthopedic surgeon experience influences radiation dose and time values. Contrary to expected, less experience is associated with lower values in some of the cases analyzed.</p>\",\"PeriodicalId\":74479,\"journal\":{\"name\":\"Porto biomedical journal\",\"volume\":\"8 3\",\"pages\":\"e218\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0e/26/pj9-8-e218.PMC10289723.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Porto biomedical journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/j.pbj.0000000000000218\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Porto biomedical journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/j.pbj.0000000000000218","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Intraoperative fluoroscopic radiation in orthopedic trauma: correlation with surgery type and surgeon experience.
Background: While fluoroscopy is widely used in orthopedic trauma surgeries, it is associated with harmful effects and should, therefore, be minimized. However, reference values for these surgeries have not been defined, and it is not known how surgeon experience affects these factors. The aims of this study were to analyze the radiation emitted and exposure time for common orthopedic trauma surgeries and to assess whether they are affected by surgeon experience.
Methods: Data from 1842 trauma orthopedic procedures were retrospectively analyzed. A total of 1421 procedures were included in the analysis. Radiation dose and time were collected to identify reference values for each surgery and compared for when the lead surgeon was a young resident, a senior resident, or a specialist.
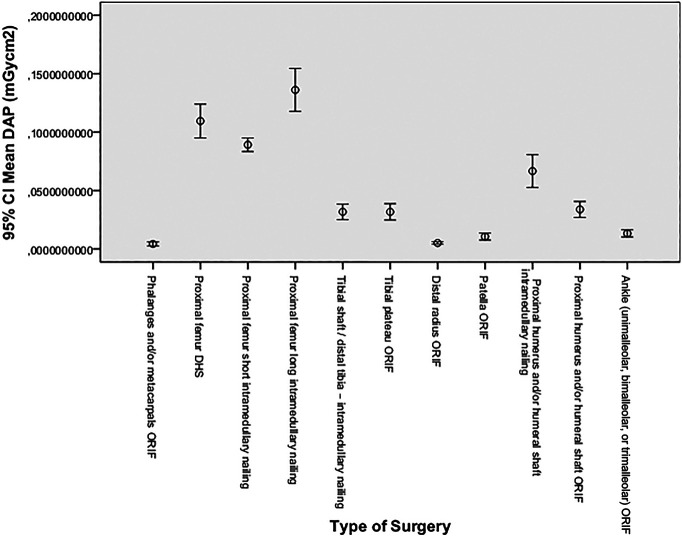
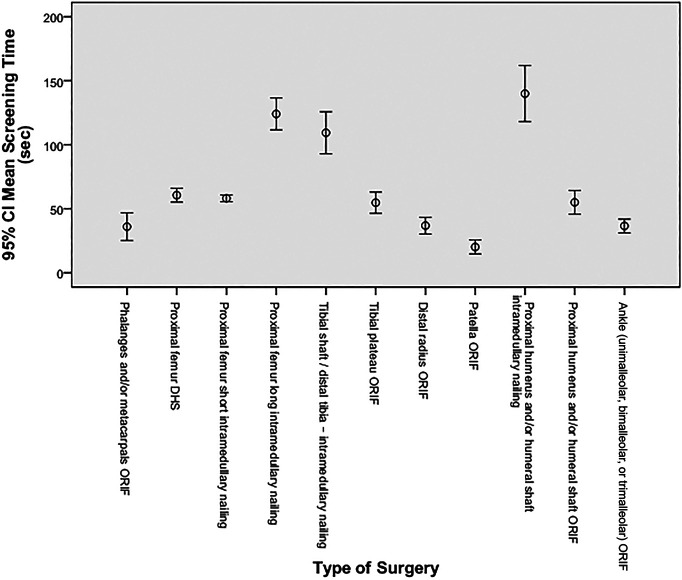
Results: The most performed surgeries requiring fluoroscopy were proximal femur short intramedullary nailing (n = 401), ankle open reduction and internal fixation (ORIF) (n = 141), distal radius ORIF (n = 125), and proximal femur dynamic hip screw (DHS) (n = 114). Surgeries using higher radiation dose were proximal femur long intramedullary nailing (mean dose area [DAP]): 1361.35 mGycm2), proximal femur DHS (1094.81 mGycm2), and proximal femur short intramedullary nailing (891.41 mGycm2). Surgeries requiring longer radiation time were proximal humerus and/or humeral shaft intramedullary nailing (02 mm:20 ss), proximal femur long intramedullary nailing (02 mm:04 ss), and tibial shaft/distal tibia intramedullary nailing (01 mm:49 ss). Senior residents required shorter radiation time when performing short intramedullary nailing of the proximal femur than young residents. Specialists required more radiation dose than residents when performing tibial nailing and tibial plateau ORIF and required longer radiation time than young residents when performing tibial nailing.
Conclusions: This study presents mean values of radiation dose and time for common orthopedic trauma surgeries. Orthopedic surgeon experience influences radiation dose and time values. Contrary to expected, less experience is associated with lower values in some of the cases analyzed.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
