澳大利亚慢性淋巴细胞白血病患者选择伊布替尼前线治疗的分子诊断检测算法的成本效益》(Cost Effectiveness of Molecular Diagnostic Testing Algorithms for the Frontline Ibrutinib Treatment Selection for Patients with Chronic Lymphocytic Leukemia in Australia)。
Martin Vu, Koen Degeling, Ella R. Thompson, Piers Blombery, David Westerman, Maarten J. IJzerman
{"title":"澳大利亚慢性淋巴细胞白血病患者选择伊布替尼前线治疗的分子诊断检测算法的成本效益》(Cost Effectiveness of Molecular Diagnostic Testing Algorithms for the Frontline Ibrutinib Treatment Selection for Patients with Chronic Lymphocytic Leukemia in Australia)。","authors":"Martin Vu, Koen Degeling, Ella R. Thompson, Piers Blombery, David Westerman, Maarten J. IJzerman","doi":"10.1007/s40258-023-00826-4","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Clinical indications for ibrutinib reimbursement in Australia should consider the inclusion of patients with chronic lymphocytic leukemia (CLL) harboring prognostically unfavorable <i>TP53/IGHV</i> genomic aberrations. This study assessed the cost effectiveness of five first-line treatment strategies in CLL for young (aged ≤ 65 years), fit patients without significant comorbidities: (1) no testing (fludarabine, cyclophosphamide and rituximab [FCR] for all), (2) test for del(17p) only, (3) test for <i>TP53</i> gene mutation status, (4) test for <i>TP53</i> and <i>IGHV</i> gene mutation status and (5) no testing (ibrutinib for all).</p><h3>Method</h3><p>A decision analytic model (decision tree and partitioned survival model) was developed from the Australian healthcare system perspective with a lifetime horizon. Comparative treatment effects were estimated from indirect treatment comparisons and survival analysis using several studies. Costs, utility and adverse events were derived from public literature sources. Deterministic and probabilistic sensitivity analyses explored the impact of modeling uncertainties on outcomes.</p><h3>Results</h3><p>Strategy 1 was associated with 5.69 quality-adjusted life-years (QALYs) and cost 458,836 Australian dollars (AUD). All other strategies had greater effectiveness but were more expensive than Strategy 1. At the willingness-to-pay (WTP) threshold of 100,000 AUD per QALY gained, Strategy 1 was most cost effective with an estimated probability of 68.8%. Strategy 4 was cost effective between thresholds 155,000–432,300 AUD per QALY gained, and Strategy 5 >432,300 AUD per QALY gained.</p><h3>Conclusion</h3><p>Population targeting using mutation testing for <i>TP53</i> and <i>IGHV</i> when performed with del(17p) testing specifically in the context of frontline ibrutinib choice does not make a cost-ineffective treatment into a cost-effective treatment.</p></div>","PeriodicalId":8065,"journal":{"name":"Applied Health Economics and Health Policy","volume":"22 1","pages":"107 - 122"},"PeriodicalIF":3.3000,"publicationDate":"2023-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10761538/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost Effectiveness of Molecular Diagnostic Testing Algorithms for the Treatment Selection of Frontline Ibrutinib for Patients with Chronic Lymphocytic Leukemia in Australia\",\"authors\":\"Martin Vu, Koen Degeling, Ella R. Thompson, Piers Blombery, David Westerman, Maarten J. IJzerman\",\"doi\":\"10.1007/s40258-023-00826-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Clinical indications for ibrutinib reimbursement in Australia should consider the inclusion of patients with chronic lymphocytic leukemia (CLL) harboring prognostically unfavorable <i>TP53/IGHV</i> genomic aberrations. This study assessed the cost effectiveness of five first-line treatment strategies in CLL for young (aged ≤ 65 years), fit patients without significant comorbidities: (1) no testing (fludarabine, cyclophosphamide and rituximab [FCR] for all), (2) test for del(17p) only, (3) test for <i>TP53</i> gene mutation status, (4) test for <i>TP53</i> and <i>IGHV</i> gene mutation status and (5) no testing (ibrutinib for all).</p><h3>Method</h3><p>A decision analytic model (decision tree and partitioned survival model) was developed from the Australian healthcare system perspective with a lifetime horizon. Comparative treatment effects were estimated from indirect treatment comparisons and survival analysis using several studies. Costs, utility and adverse events were derived from public literature sources. Deterministic and probabilistic sensitivity analyses explored the impact of modeling uncertainties on outcomes.</p><h3>Results</h3><p>Strategy 1 was associated with 5.69 quality-adjusted life-years (QALYs) and cost 458,836 Australian dollars (AUD). All other strategies had greater effectiveness but were more expensive than Strategy 1. At the willingness-to-pay (WTP) threshold of 100,000 AUD per QALY gained, Strategy 1 was most cost effective with an estimated probability of 68.8%. Strategy 4 was cost effective between thresholds 155,000–432,300 AUD per QALY gained, and Strategy 5 >432,300 AUD per QALY gained.</p><h3>Conclusion</h3><p>Population targeting using mutation testing for <i>TP53</i> and <i>IGHV</i> when performed with del(17p) testing specifically in the context of frontline ibrutinib choice does not make a cost-ineffective treatment into a cost-effective treatment.</p></div>\",\"PeriodicalId\":8065,\"journal\":{\"name\":\"Applied Health Economics and Health Policy\",\"volume\":\"22 1\",\"pages\":\"107 - 122\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2023-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10761538/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Applied Health Economics and Health Policy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://link.springer.com/article/10.1007/s40258-023-00826-4\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Applied Health Economics and Health Policy","FirstCategoryId":"3","ListUrlMain":"https://link.springer.com/article/10.1007/s40258-023-00826-4","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
Cost Effectiveness of Molecular Diagnostic Testing Algorithms for the Treatment Selection of Frontline Ibrutinib for Patients with Chronic Lymphocytic Leukemia in Australia
Background
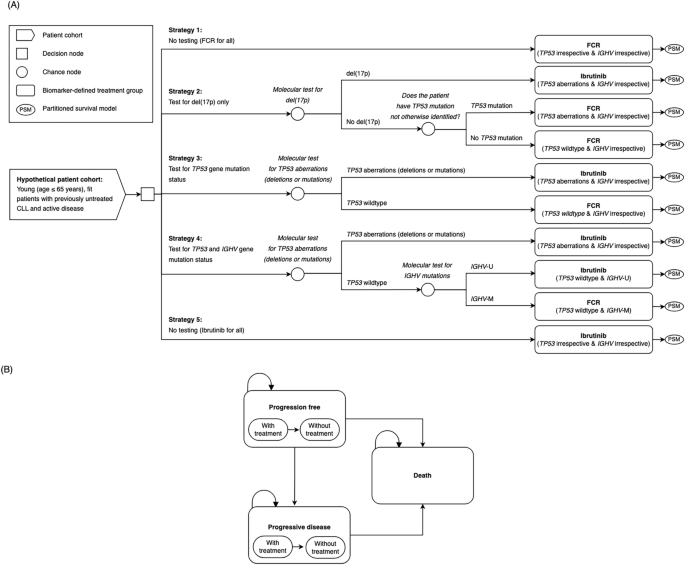
Clinical indications for ibrutinib reimbursement in Australia should consider the inclusion of patients with chronic lymphocytic leukemia (CLL) harboring prognostically unfavorable TP53/IGHV genomic aberrations. This study assessed the cost effectiveness of five first-line treatment strategies in CLL for young (aged ≤ 65 years), fit patients without significant comorbidities: (1) no testing (fludarabine, cyclophosphamide and rituximab [FCR] for all), (2) test for del(17p) only, (3) test for TP53 gene mutation status, (4) test for TP53 and IGHV gene mutation status and (5) no testing (ibrutinib for all).
Method
A decision analytic model (decision tree and partitioned survival model) was developed from the Australian healthcare system perspective with a lifetime horizon. Comparative treatment effects were estimated from indirect treatment comparisons and survival analysis using several studies. Costs, utility and adverse events were derived from public literature sources. Deterministic and probabilistic sensitivity analyses explored the impact of modeling uncertainties on outcomes.
Results
Strategy 1 was associated with 5.69 quality-adjusted life-years (QALYs) and cost 458,836 Australian dollars (AUD). All other strategies had greater effectiveness but were more expensive than Strategy 1. At the willingness-to-pay (WTP) threshold of 100,000 AUD per QALY gained, Strategy 1 was most cost effective with an estimated probability of 68.8%. Strategy 4 was cost effective between thresholds 155,000–432,300 AUD per QALY gained, and Strategy 5 >432,300 AUD per QALY gained.
Conclusion
Population targeting using mutation testing for TP53 and IGHV when performed with del(17p) testing specifically in the context of frontline ibrutinib choice does not make a cost-ineffective treatment into a cost-effective treatment.
期刊介绍:
Applied Health Economics and Health Policy provides timely publication of cutting-edge research and expert opinion from this increasingly important field, making it a vital resource for payers, providers and researchers alike. The journal includes high quality economic research and reviews of all aspects of healthcare from various perspectives and countries, designed to communicate the latest applied information in health economics and health policy.
While emphasis is placed on information with practical applications, a strong basis of underlying scientific rigor is maintained.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
