Shahab Masoumi, Ahmad Separham, Razieh Parizad, Samira Jafarisis, Marjan Assefi
{"title":"双左前降支:临床综述和介入治疗。","authors":"Shahab Masoumi, Ahmad Separham, Razieh Parizad, Samira Jafarisis, Marjan Assefi","doi":"10.18502/jthc.v18i2.13326","DOIUrl":null,"url":null,"abstract":"<p><p>Congenital coronary artery anomalies are relatively rare, occurring in approximately 0.6%-1.3% of cases undergoing coronary angiography. Among these anomalies, a unique cardiac abnormality known as a dual left anterior descending artery (LAD) stands out. A dual LAD is characterized by the presence of 2 LADs in the anterior interventricular sulcus. This structural deviation consists of a shorter LAD that terminates high in the anterior interventricular sulcus and a longer LAD that extends to the distal sulcus, supplying blood to the cardiac apex. Percutaneous procedures on dual LADs are even less frequent. We describe a 53-year-old woman with typical burning chest pain, ST-elevation in leads I and aVL, and positive troponin I enzyme. Coronary angiography revealed a thrombotic lesion with 99% stenosis at the proximal part of the LAD. The main LAD originated properly from the left coronary cusp, and the remainder of its course was supplied by a second branch originating from the right coronary cusp. Computed tomography angiography and echocardiography were performed for the LAD course. The patient was discharged after an uneventful 1-week hospital stay. Our case is particularly noteworthy for several reasons. Firstly, this dual LAD anomaly is uncommon, and patients with dual LADs less frequently have a ramus artery. Secondly, there have been only a few documented cases of percutaneous transluminal coronary angioplasty performed on short LADs. The key takeaway from this scintillating case study is the significance of identifying the artery responsible for blood supply to the cardiac apex.</p>","PeriodicalId":39149,"journal":{"name":"Journal of Tehran University Heart Center","volume":"18 2","pages":"146-150"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f7/c7/JTHC-18-146.PMC10459347.pdf","citationCount":"0","resultStr":"{\"title\":\"Dual Left Anterior Descending Artery: Clinical Overview and Interventional Management.\",\"authors\":\"Shahab Masoumi, Ahmad Separham, Razieh Parizad, Samira Jafarisis, Marjan Assefi\",\"doi\":\"10.18502/jthc.v18i2.13326\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Congenital coronary artery anomalies are relatively rare, occurring in approximately 0.6%-1.3% of cases undergoing coronary angiography. Among these anomalies, a unique cardiac abnormality known as a dual left anterior descending artery (LAD) stands out. A dual LAD is characterized by the presence of 2 LADs in the anterior interventricular sulcus. This structural deviation consists of a shorter LAD that terminates high in the anterior interventricular sulcus and a longer LAD that extends to the distal sulcus, supplying blood to the cardiac apex. Percutaneous procedures on dual LADs are even less frequent. We describe a 53-year-old woman with typical burning chest pain, ST-elevation in leads I and aVL, and positive troponin I enzyme. Coronary angiography revealed a thrombotic lesion with 99% stenosis at the proximal part of the LAD. The main LAD originated properly from the left coronary cusp, and the remainder of its course was supplied by a second branch originating from the right coronary cusp. Computed tomography angiography and echocardiography were performed for the LAD course. The patient was discharged after an uneventful 1-week hospital stay. Our case is particularly noteworthy for several reasons. Firstly, this dual LAD anomaly is uncommon, and patients with dual LADs less frequently have a ramus artery. Secondly, there have been only a few documented cases of percutaneous transluminal coronary angioplasty performed on short LADs. The key takeaway from this scintillating case study is the significance of identifying the artery responsible for blood supply to the cardiac apex.</p>\",\"PeriodicalId\":39149,\"journal\":{\"name\":\"Journal of Tehran University Heart Center\",\"volume\":\"18 2\",\"pages\":\"146-150\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f7/c7/JTHC-18-146.PMC10459347.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Tehran University Heart Center\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.18502/jthc.v18i2.13326\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Tehran University Heart Center","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jthc.v18i2.13326","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Dual Left Anterior Descending Artery: Clinical Overview and Interventional Management.
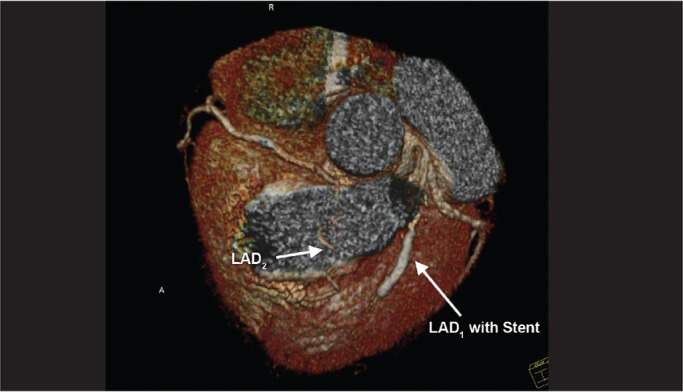
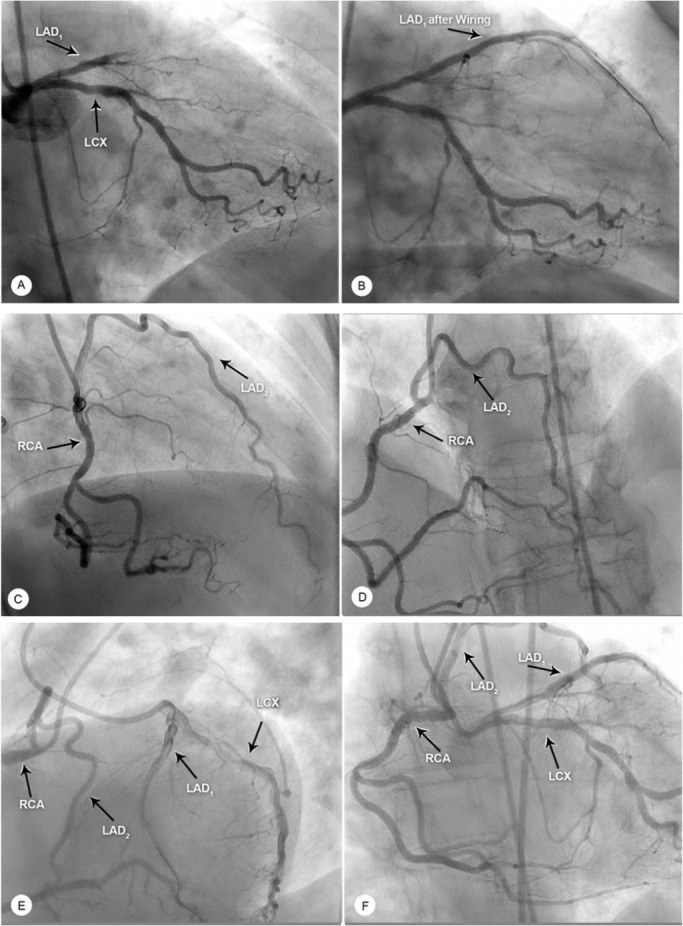
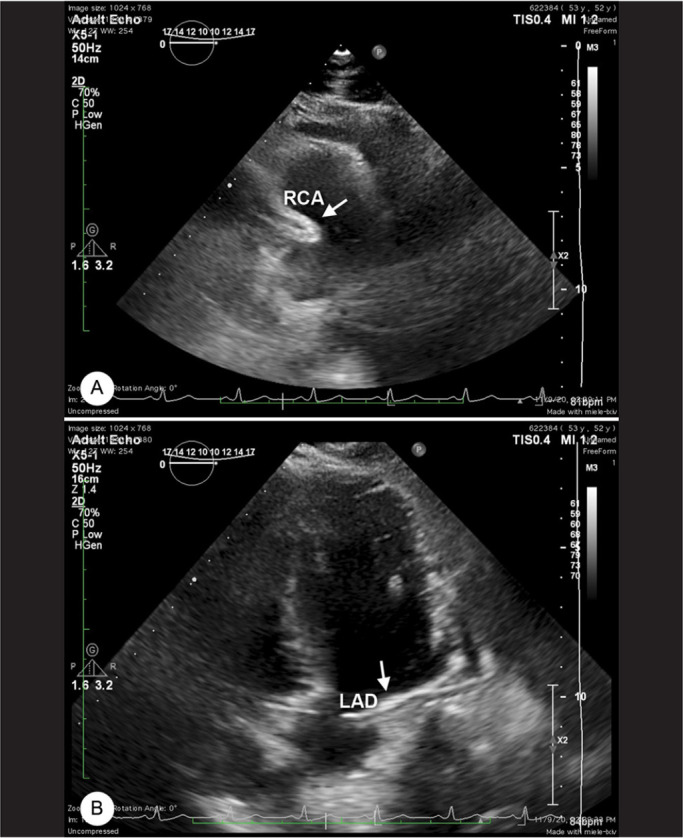
Congenital coronary artery anomalies are relatively rare, occurring in approximately 0.6%-1.3% of cases undergoing coronary angiography. Among these anomalies, a unique cardiac abnormality known as a dual left anterior descending artery (LAD) stands out. A dual LAD is characterized by the presence of 2 LADs in the anterior interventricular sulcus. This structural deviation consists of a shorter LAD that terminates high in the anterior interventricular sulcus and a longer LAD that extends to the distal sulcus, supplying blood to the cardiac apex. Percutaneous procedures on dual LADs are even less frequent. We describe a 53-year-old woman with typical burning chest pain, ST-elevation in leads I and aVL, and positive troponin I enzyme. Coronary angiography revealed a thrombotic lesion with 99% stenosis at the proximal part of the LAD. The main LAD originated properly from the left coronary cusp, and the remainder of its course was supplied by a second branch originating from the right coronary cusp. Computed tomography angiography and echocardiography were performed for the LAD course. The patient was discharged after an uneventful 1-week hospital stay. Our case is particularly noteworthy for several reasons. Firstly, this dual LAD anomaly is uncommon, and patients with dual LADs less frequently have a ramus artery. Secondly, there have been only a few documented cases of percutaneous transluminal coronary angioplasty performed on short LADs. The key takeaway from this scintillating case study is the significance of identifying the artery responsible for blood supply to the cardiac apex.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
